A positive pregnancy test can bring joy and panic at the same time when ADHD is already part of daily life. Many women reach for the same questions within minutes. Should the medication stop today? Will untreated symptoms make pregnancy harder? Is there a middle path that protects both maternal functioning and fetal health?
That tension is real. The conversation around ADHD medication for pregnant women often gets flattened into a simple safe-or-unsafe debate, but clinical care rarely works that way. The more useful question is whether continuing, tapering, switching, or pausing treatment makes the most sense for one person's symptom burden, work demands, home responsibilities, medical history, and pregnancy course.
A review of dispensing data found that prescribing during pregnancy is still uncommon, ranging from 0.07 to 6.01 per 1,000 pregnancies, and about 60% of women with ADHD discontinue medication during pregnancy, which reflects how much uncertainty still shapes these decisions according to this systematic review on ADHD-medication prescribing in pregnancy. Women deserve clearer guidance than fear-based advice.
Table of Contents
- The Pregnancy and ADHD Dilemma
- Why Managing ADHD in Pregnancy Matters
- ADHD Medication Safety An Evidence-Based Overview
- Navigating Risks by Trimester
- Your Preconception and Pregnancy Care Plan
- Integrative Support Beyond Medication
- Postpartum Care and Breastfeeding with ADHD Meds
The Pregnancy and ADHD Dilemma
A common pattern is easy to recognize. A woman learns she's pregnant, looks at her stimulant or non-stimulant bottle, and feels cornered by two risks at once. One risk is fetal exposure. The other is suddenly losing the treatment that helps her stay organized, drive safely, show up to work, remember appointments, and regulate emotion.

That moment often happens before she's seen her OB clinician or psychiatric prescriber. It's also when internet advice becomes least helpful. Blanket warnings can make women feel as if any choice they make is reckless, even though pregnancy care usually involves weighing competing priorities rather than avoiding all uncertainty.
For women already noticing how hormones affect concentration, impulsivity, mood, and sleep, this can feel especially destabilizing. Resources on ADHD in women and integrative treatment options can help frame the broader picture, because pregnancy doesn't erase ADHD. It changes how symptoms interact with the body, daily routines, and medical decisions.
Why this decision feels so charged
The emotional pressure makes sense. Pregnancy tends to increase a sense of responsibility, and ADHD can make it harder to tolerate ambiguity. Many women want a clean answer right away. Medicine often can't offer one.
What it can offer is a structured process. That process starts by identifying the trade-off. Stopping medication may reduce exposure, but it can also reduce functioning. Continuing medication may preserve stability, but it may call for closer monitoring and a more detailed plan.
Practical rule: The strongest pregnancy decisions usually come from individualized risk-benefit review, not reflexively stopping treatment on day one.
A better frame than safe or unsafe
The question isn't whether all ADHD medications are universally safe or unsafe in pregnancy. The question is which option creates the most manageable risk profile for a specific patient at a specific point in pregnancy.
That approach is more compassionate and more clinically honest. It respects both maternal well-being and fetal health. It also recognizes that women don't need shame. They need clear evidence, careful monitoring, and a provider who can discuss trade-offs without oversimplifying them.
Why Managing ADHD in Pregnancy Matters
A patient learns she is pregnant on Tuesday and stops her ADHD medication that same day. By the end of the week, she is missing emails from her obstetric office, forgetting meals, arriving late to work, and crying because simple tasks suddenly feel unmanageable. I see versions of this often in practice. The problem is not a lack of commitment to the pregnancy. The problem is that untreated ADHD can quickly interfere with the routines and follow-through that pregnancy care depends on.
Stopping treatment may lower fetal medication exposure. It can also raise another set of risks if symptoms return hard and fast. Shared decision-making matters here because the actual question is not whether treatment is good or bad in the abstract. The question is what helps a specific woman stay safest and most functional during pregnancy.
Untreated symptoms can interfere with pregnancy care
ADHD affects more than focus. It often affects initiation, time management, emotional control, sleep, and the ability to keep track of changing instructions. During pregnancy, those weaknesses can show up in practical ways that matter.
Common examples include:
- Missed prenatal tasks: forgetting appointments, delaying labs, misplacing paperwork, or running out of prescribed medications before requesting refills
- Poor routine stability: inconsistent meals, hydration, sleep timing, and other habits that support day-to-day health
- Impulsive decision-making under stress: difficulty slowing down around driving, work demands, conflict, spending, or substance use
- More psychiatric symptoms: anxiety, low mood, irritability, and overwhelm often get harder to manage when ADHD is untreated
For some women, the biggest issue is not productivity. It is safety. Distracted driving, medication mix-ups, missed blood pressure checks, and difficulty responding to new medical instructions can become more likely when symptoms are poorly controlled.
Maternal functioning is part of the risk-benefit analysis
Maternal functioning belongs in the conversation. A woman who cannot reliably organize meals, attend visits, communicate symptoms, or manage daily responsibilities is not automatically better off because she stopped a prescription.
This is why I encourage patients to review impairment in concrete terms. Can she get to appointments on time? Can she remember prenatal guidance from one visit to the next? Can she work safely, parent safely, and keep a stable routine at home? Those answers often shape the treatment plan more than fear-based labels about medication.
Women comparing ADHD medication options and treatment considerations often find that side effect burden also matters during pregnancy, especially if nausea, appetite changes, insomnia, or blood pressure concerns are already in the picture. Qaly's ADHD medication guide gives a useful overview of common adverse effects that may need closer review in a prenatal setting.
Clinical reviews have also noted that women with more impairing ADHD may benefit from continuing treatment after an individualized discussion of symptom burden, obstetric factors, psychiatric history, and medication type, as described in this review of ADHD medications in pregnancy and lactation.
A careful plan may still involve tapering, switching, or pausing medication. It may also involve continuing treatment with monitoring. Good care comes from weighing both sides clearly, then choosing the option that best supports the mother's functioning and the pregnancy overall.
ADHD Medication Safety An Evidence-Based Overview
The strongest current evidence is more reassuring than many women expect, especially regarding major malformations and miscarriage for specific medications. That doesn't mean every drug has the same data quality or that all pregnancy risks disappear. It means the evidence doesn't support a simplistic alarmist view.
Women who search for an online psychiatrist, a psychiatric nurse practitioner, or telepsychiatry in Pennsylvania are often trying to sort through conflicting messages quickly. The most helpful clinical conversations separate structural birth-defect concerns from later obstetric concerns such as blood pressure, placental function, fetal growth, and delivery timing.
What current evidence supports
A 2024 systematic review and meta-analysis covering 16.5 million pregnant women found that methylphenidate and atomoxetine were not associated with a significant increase in congenital anomalies or miscarriages in JAMA Network Open's meta-analysis on ADHD medication exposure in pregnancy.
A separate large review of pregnancy outcomes reported similar findings. Across 5 studies, the odds ratio for congenital anomalies among exposed versus unexposed women with ADHD was 1.14 (95% CI 0.83 to 1.55), and compared with the general pregnant population the odds ratios were 1.19 (95% CI 0.93 to 1.53) for congenital anomalies and 1.05 (95% CI 0.81 to 1.37) for miscarriage in this perinatal outcomes review summarized by AAP Grand Rounds.
Those pooled estimates sit close to 1.0, which means the data didn't show a clear increase in risk for those outcomes. For patients, that changes the conversation. It moves the focus away from “all exposure is dangerous” and toward “which risks remain most relevant for this medication, trimester, and symptom profile.”
A practical comparison by medication class
| Medication Class | Common Agents | Key Considerations based on Current Evidence |
|---|---|---|
| Stimulants | Methylphenidate, amphetamine-based medications | Malformation data are more reassuring than many patients expect, but later-pregnancy monitoring may matter more because some studies suggest signals involving blood pressure, preterm birth, and neonatal observation rather than structural defects. |
| Non-stimulants | Atomoxetine, bupropion | Atomoxetine has reassuring data regarding congenital anomalies and miscarriage in pooled analyses. For other non-stimulants, evidence is more variable, so decisions often depend on how well the medication works for the patient and how much pregnancy-specific data exist. |
Patients often ask whether they should compare side-effect profiles before pregnancy visits. A plain-language resource like Qaly's ADHD medication guide can help women review common medication differences before they talk through pregnancy-specific planning with a prescriber.
For women seeking adult ADHD treatment, ADHD medication management, women's mental health care, or virtual psychiatric care, medication review should include more than the drug name. It should cover dose, symptom rebound, appetite, sleep, blood pressure, prior pregnancy history, and whether the medication supports baseline functioning enough to justify continued exposure.
Clinical evaluation for ADHD medication management can support that kind of detailed review when decisions need to be revisited across pregnancy rather than made once and forgotten.
Navigating Risks by Trimester
Pregnancy risk isn't static. Timing matters. A medication that raises one concern early in pregnancy may raise a different concern later, which is why trimester-specific counseling is more useful than one blanket statement for the entire pregnancy.
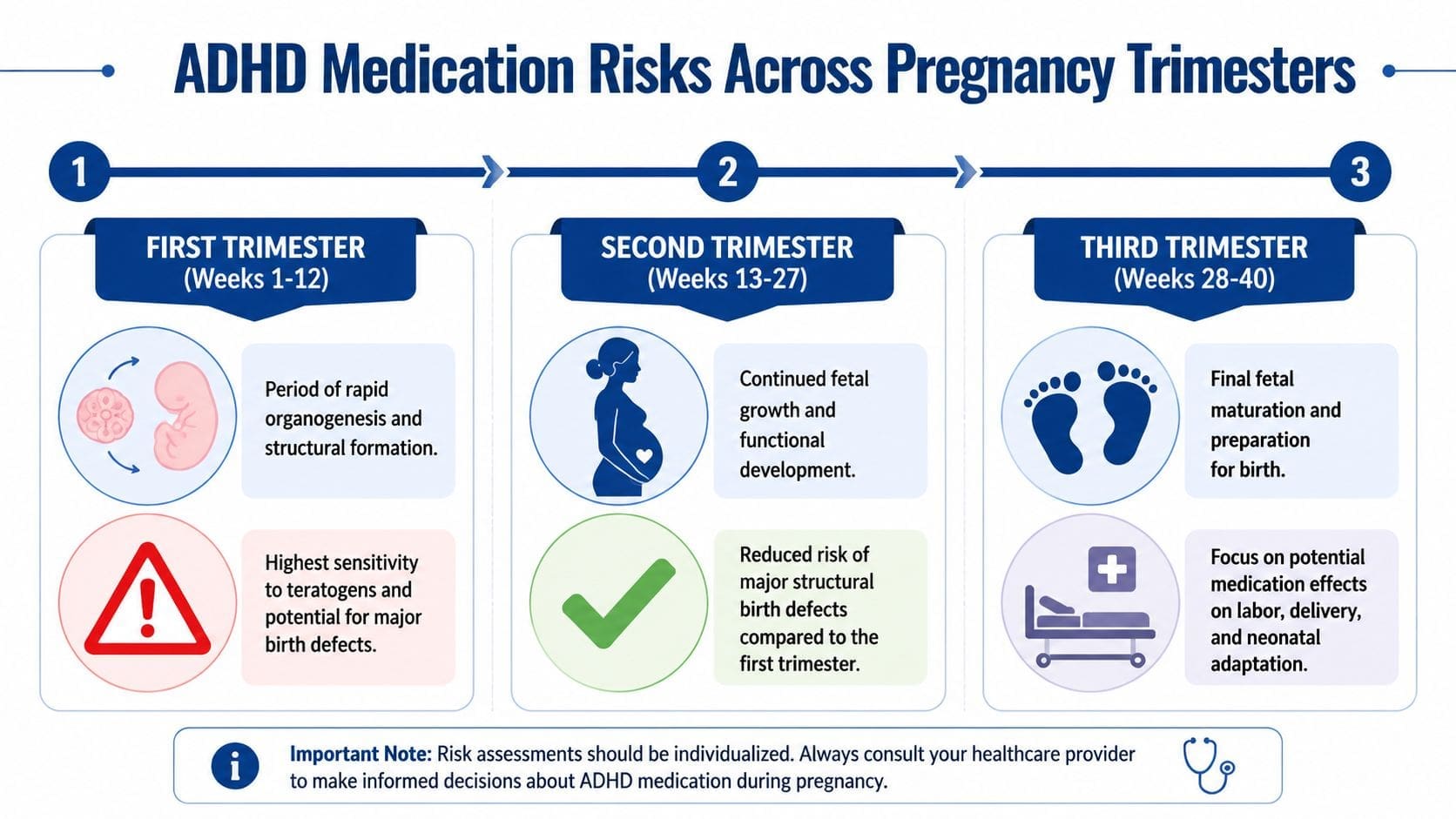
First trimester concerns
The first trimester gets the most attention because it includes organogenesis, the phase when fetal structures are forming. That's why so many medication discussions focus on congenital anomalies. Women who discover pregnancy after a period of early exposure often fear they've already caused harm, and that's where precise counseling matters.
Current evidence for methylphenidate and atomoxetine is more reassuring than older public messaging suggests, but first-trimester exposure still deserves individualized review. Some guidance also notes a small cardiac-safety signal with methylphenidate, which is one reason prescribers may discuss whether dose changes, closer obstetric follow-up, or medication adjustments make sense.
Later pregnancy monitoring
In the second and third trimesters, the main concerns often shift away from structural defects and toward maternal and perinatal outcomes. A stimulant that didn't raise clear malformation concerns may still call for blood pressure checks, fetal growth monitoring, and attention to delivery timing.
One review reported an adjusted odds ratio of 1.29 for preeclampsia with stimulant use in pregnancy, while other datasets found small increases in preterm birth and NICU admission in this 2023 review summary on stimulant-associated obstetric risk. That pattern supports practical monitoring rather than panic.
A trimester-based plan may include:
- Early pregnancy: Confirm exposure timing, assess whether symptoms are mild enough for a pause or taper, and review prior medication response.
- Mid-pregnancy: Reassess work function, nutrition, sleep, and emotional regulation if symptoms are returning.
- Late pregnancy: Watch maternal blood pressure, follow fetal growth as recommended by obstetric care, and discuss whether dose timing needs adjustment as delivery approaches.
Blood pressure, fetal growth, and delivery planning often matter more in late pregnancy than repeating a generic question about whether the medication is “safe.”
Women who are specifically evaluating lisdexamfetamine can review Vyvanse and pregnancy considerations as part of a medication-specific discussion, since practical decisions often depend on the exact agent rather than the ADHD label alone.
Your Preconception and Pregnancy Care Plan
A common preconception visit sounds like this. “I can function at work with my medication, but I miss meals, lose track of appointments, and feel unsafe driving without it. If I'm trying to get pregnant, what do I do now?”
That is the right question. The goal is not to force every woman into staying on medication or stopping it. The goal is to build a plan that weighs fetal exposure against the practical risks of untreated ADHD, then revisit that plan as pregnancy progresses.
If pregnancy is planned, start before conception. If the pregnancy test is already positive, start now. In both situations, the first step is the same. Clarify what the medication improves, what happens when it is lowered or stopped, and which symptoms create the most risk in daily life.
Questions that shape the decision
The most useful treatment plans are specific. I want to know where ADHD shows up when a patient is unmedicated, because “I'm more distracted” means something very different from missing prenatal visits, making driving errors, forgetting to eat, or struggling to care for other children.
Key questions include:
- How impairing are symptoms without medication? Mild forgetfulness and severe executive dysfunction do not carry the same pregnancy risks.
- What happens with skipped doses or prior tapers? Past experience often predicts whether a medication reduction is realistic.
- Which target symptoms matter most? Attention, impulsivity, emotional reactivity, binge eating, task completion, and wakefulness can each affect the plan.
- What other supports are in place? Therapy, partner support, flexible work, childcare help, and structured routines can lower the pressure on medication alone.
- What medical factors may change the plan? Blood pressure history, nausea, weight loss, insomnia, anxiety, and prior pregnancy complications all matter.
What shared decision-making looks like in practice
Shared decision-making is a clinical process, not a checkbox on a consent form. One woman may decide that a taper is reasonable because her symptoms are manageable, her work is flexible, and she has strong support at home. Another may decide that continuing medication at the lowest effective dose is safer overall because untreated symptoms put her job, nutrition, driving, or parenting at risk.
Plans also change. A patient may feel stable early in pregnancy and then struggle later when fatigue, sleep disruption, or work demands increase. Another may reduce medication successfully but need a clear restart plan if functioning drops.
A practical care plan usually includes five parts:
- Medication review. Confirm the current medication, dose, timing, benefits, side effects, and any previous attempts to stop or switch.
- Function review. Look at work performance, household safety, driving, appointment follow-through, eating patterns, and emotional regulation.
- Monitoring roles. Decide what the psychiatric clinician will follow, what the OB team will follow, and when those updates need to be shared.
- Adjustment options. Set clear next steps if symptoms worsen, side effects appear, or pregnancy-related concerns change the risk-benefit balance.
- Postpartum preparation. Make decisions before delivery about sleep protection, feeding plans, relapse risk, and medication timing after birth.
Some women also want a broader review of contributing factors such as sleep quality, iron status, thyroid function, anxiety, or GI symptoms when choosing gut-brain axis support. Those steps do not replace psychiatric care, but they can sharpen the treatment plan.
For patients who need formal psychiatric evaluation or medication follow-up during this period, knowing when to see a psychiatrist for medication planning in pregnancy can help avoid last-minute decisions after symptoms have already become harder to manage. Integrative Psychiatry of America provides telehealth psychiatric evaluation and medication management by psychiatric nurse practitioners, which can support coordinated planning across preconception, pregnancy, and postpartum care.
Integrative Support Beyond Medication
Medication is one tool. For some pregnant women, it remains part of treatment. For others, it becomes a smaller part. Either way, symptom management usually improves when behavioral and lifestyle supports are added deliberately rather than left as vague advice.
Non-medication supports that help
Some supports work because they reduce cognitive load. Others stabilize mood, sleep, or energy. The most practical options include:
- CBT and skills-based therapy: Helpful for task initiation, emotional regulation, and all-or-nothing thinking.
- ADHD coaching or structured planning systems: External reminders, visual schedules, and weekly check-ins can compensate for executive dysfunction.
- Exercise that fits pregnancy: Walking, prenatal yoga, and other clinician-approved movement can support focus, stress regulation, and sleep.
- Nutrition routines: Regular meals and protein-forward snacks can reduce the crash that makes attention and irritability worse.
- Mindfulness practices: Brief breathing work and body-based grounding can help women slow impulsive reactions when overwhelmed.
A growing number of patients are also interested in nutrition and digestion because ADHD symptoms often worsen when sleep, appetite, and energy become erratic. For readers exploring that angle, this overview of choosing gut-brain axis support offers a useful framework for understanding how some people think about broader brain-body support, though pregnancy-specific supplement choices should always be reviewed with a clinician.
This short video offers another practical perspective on supportive strategies during pregnancy and ADHD care.
Women who want more structure around food, energy regulation, and ADHD can also review nutrition guidance for pregnant women with ADHD. That kind of support can be especially useful when medication is reduced, appetite changes, or nausea disrupts normal routines.
Postpartum Care and Breastfeeding with ADHD Meds
Delivery doesn't end the decision-making process. In many ways, the postpartum period is when ADHD symptoms become harder to predict. Sleep loss, hormonal shifts, feeding demands, and round-the-clock task switching can strain attention and emotional regulation quickly.
Planning for the fourth trimester
Recent guidance emphasizes that ADHD medication decisions should include a postpartum plan, not just a pregnancy plan. Newer meta-analytic work found no increase in long-term neurodevelopmental disorders in exposed offspring, while practical questions remain around lactation compatibility, infant monitoring, and drug-specific feeding decisions in this clinician guidance document on ADHD care in pregnancy and postpartum.
The breastfeeding conversation often sounds similar to the pregnancy conversation. It's about trade-offs. A small amount of medication exposure through breast milk may need to be weighed against the benefits of breastfeeding and the mother's ability to function safely and consistently. Drug choice, dose timing, infant age, and pediatric follow-up all matter.
Practical postpartum planning often includes:
- Restart timing: Decide before delivery whether medication will resume immediately, after milk supply is established, or only if symptoms return.
- Infant observation: Review what to watch for, such as feeding difficulty, irritability, sleep disruption, or poor weight gain.
- Maternal symptom tracking: Watch for ADHD rebound, depression, anxiety, and cognitive overload.
- Coordination with pediatric and obstetric care: Make sure all clinicians know the medication plan.
Women who want a broader explanation of how the brain changes after childbirth may find this article on postpartum brain changes helpful as background reading. It isn't specific to ADHD medication, but it can make the postpartum experience feel less confusing and less personal.
If pregnancy is changing how ADHD treatment needs to work, support is available through Integrative Psychiatry of America. A psychiatric nurse practitioner can help review symptom severity, medication options, trimester-specific concerns, non-medication supports, and postpartum planning so the next step feels informed rather than rushed.

