A positive pregnancy test can turn a routine ADHD refill question into an urgent, emotional one. Many adults taking Vyvanse feel two fears at the same time. One is fear of harming the pregnancy. The other is fear of losing the focus, follow-through, and emotional steadiness they rely on to function at work, at home, and in medical care.
That tension is real. It doesn't mean anyone has made a mistake, and it doesn't mean the answer is automatically to stop medication overnight. In psychiatric practice, vyvanse pregnancy decisions work best when they are handled as a coordinated plan, not a panic response.
Table of Contents
- The Big Question When You're Expecting with ADHD
- Why Stopping Vyvanse Isn't Always a Simple Choice
- Vyvanse and Pregnancy Safety The Current Evidence
- Making an Informed Decision with Your Provider
- Alternatives and Management Strategies During Pregnancy
- Navigating Postpartum Care and Breastfeeding on Vyvanse
- How to Get Expert Support for Your Pregnancy Journey
The Big Question When You're Expecting with ADHD
A common scenario looks like this. A patient has been stable on Vyvanse, finds out she's pregnant, and immediately starts searching for answers late at night. Within minutes, she's reading conflicting advice, feeling guilty, and wondering whether to skip the next dose before talking to anyone.
That first impulse is understandable, but it often creates more problems than it solves. ADHD doesn't disappear during pregnancy. If anything, the executive function demands increase quickly. There are prenatal appointments to remember, supplements to take consistently, sleep changes to manage, and work responsibilities that usually don't pause because someone is newly expecting.
What makes this decision hard
Vyvanse pregnancy decisions are rarely simple because the question isn't only "Is medication risky?" The true question is "What happens if treatment continues, and what happens if treatment stops?" Both sides matter.
Some patients have mild symptoms and can taper with support. Others depend on stimulant treatment to drive safely, keep a job, manage other children, or function in a structured profession. For women with ADHD, this often sits inside a larger picture of mood regulation, sleep disruption, anxiety, and overload. Support like integrative ADHD care for women can help frame the issue in a whole-person way rather than as a medication-only question.
Pregnancy planning for ADHD works better when shame is removed from the conversation and functioning is treated as a health issue.
What patients need most early on
The most useful first step is a calm review of the facts, current symptoms, and pregnancy timeline. That means checking how severe ADHD symptoms are without medication, what trimester the patient is in, whether blood pressure has ever been an issue, and who is coordinating care between psychiatry and obstetrics.
This approach doesn't produce a one-size-fits-all answer. It produces a safer one.
Why Stopping Vyvanse Isn't Always a Simple Choice
Vyvanse, or lisdexamfetamine, is a stimulant medication used for ADHD. For many adults, it improves attention, task initiation, organization, follow-through, and the ability to regulate frustration before it turns into impulsive decisions. That matters in pregnancy because routine, planning, and self-management suddenly become even more important.
The outside view of ADHD can be misleading. People often assume it's mostly distractibility. In practice, untreated symptoms can affect medication adherence, meal planning, transportation, paperwork, appointment attendance, work reliability, and relationship stability. A patient may look "high functioning" from the outside while spending enormous effort just to hold a normal day together.
Why some patients feel dramatically worse off medication
When stimulant treatment is removed too quickly, some patients don't just lose focus. They lose structure. They may sleep at irregular times, miss calls from the OB office, forget to eat, or become less consistent with prenatal habits that protect maternal and fetal health.
This is why a simplistic "just stop" recommendation often fails in real life. If someone had significant ADHD symptoms before pregnancy, those symptoms usually remain relevant during pregnancy. For many adults seeking online ADHD medication support, stimulant treatment isn't about productivity in a superficial sense. It's about basic functioning.
The pregnancy concern is more specific than many people realize
Mechanistically, Vyvanse is an amphetamine stimulant, so the main pregnancy concerns are pharmacologic effects on maternal vasculature and uterine activity rather than a proven pattern of major malformations, as described in this review of Vyvanse reproductive health concerns. Amphetamine exposure has been associated with vasoconstriction that may reduce placental-fetal perfusion and stimulation of uterine contractions that can increase preterm birth risk in that same source.
Clinical reality: The decision often isn't between a perfect option and a dangerous option. It's between two imperfect options that carry different kinds of risk.
That distinction matters. A patient deciding about lisdexamfetamine in pregnancy needs more than fear-based advice. She needs a realistic understanding of what the medication does for her, what its pregnancy concerns are, and what daily life is likely to look like if the plan changes.
Vyvanse and Pregnancy Safety The Current Evidence
The current evidence gives us a more nuanced picture than many patients expect. In practice, the central question is usually not whether Vyvanse has been tied to a clear, consistent pattern of major birth defects. The harder question is whether continuing treatment changes the chances of complications such as preterm delivery, lower birth weight, or hypertensive disorders, and how those risks compare with the risks of untreated ADHD for that specific patient.
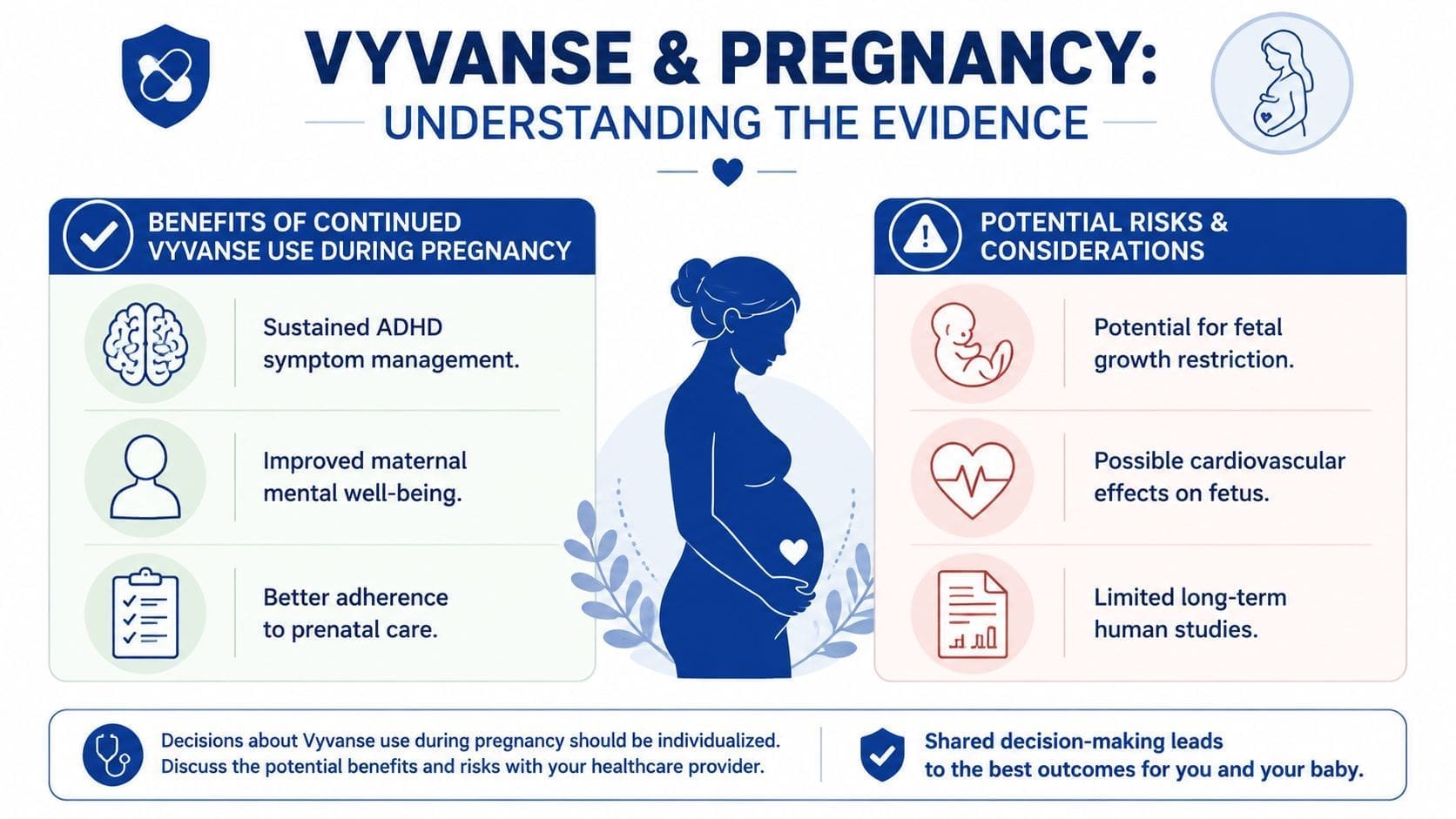
A summary of a 2023 JAMA Psychiatry analysis of more than 5,000 stimulant-exposed pregnancies reported no significant increase in major birth defects with amphetamine-based medications such as Vyvanse, while also noting possible modest elevations in outcomes such as preterm delivery, low birth weight, and gestational hypertension, according to this evidence summary on Vyvanse and pregnancy safety.
What clinicians can say with reasonable confidence
For counseling purposes, that is reassuring in one specific area. Larger observational datasets have not shown a strong teratogenic signal for prescription amphetamine stimulants as a class. For many pregnant patients, that changes the discussion from fear about major malformations to a more grounded review of maternal blood pressure, fetal growth, sleep, nutrition, and day-to-day functioning.
There is still uncertainty. Much of what we know comes from observational research, which means the studies can be affected by differences in baseline health, psychiatric severity, substance use, nutrition, and prenatal care. A patient taking Vyvanse during pregnancy may differ in important ways from a patient who stops medication before conception.
Where concern still exists
The main concerns in the literature are perinatal and obstetric outcomes rather than a single dramatic birth-defect pattern. Earlier in this article, we reviewed data suggesting higher rates of preterm birth and lower birth weight in some exposed groups. Those findings do not prove that Vyvanse directly caused the outcome in every case, but they are enough to justify closer monitoring and a careful prescribing plan.
Lisdexamfetamine-specific data also remain limited. Vyvanse is a prodrug of dextroamphetamine, so risk estimates are often drawn from broader amphetamine data rather than large studies focused only on lisdexamfetamine. That matters in real clinical care. It means we should be honest about what is well supported, what is inferred from related medications, and where the evidence still leaves room for judgment.
How we interpret this in practice
At Integrative Psychiatry of America, we usually organize the evidence into three clinical buckets:
- Major malformations: Current population-level data is generally reassuring and does not show a clear, repeated signal for a large increase in major birth defects.
- Pregnancy course: Some studies suggest possible increases in problems such as preterm birth, lower birth weight, or gestational hypertension, especially when other maternal risk factors are present.
- Maternal functioning: The safety discussion is incomplete if it ignores what happens when severe ADHD symptoms return. Missed prenatal visits, poor sleep routines, disorganized medication use, driving problems, and difficulty maintaining nutrition can all become part of the risk picture.
That whole-person view matters. A pregnant patient with mild ADHD symptoms and strong support at home may reasonably choose to taper off Vyvanse. A patient with severe executive dysfunction, a history of accidents, or major impairment at work or in parenting may face a very different set of risks.
For patients weighing these options, our guide to ADHD medication during pregnancy, including stimulants and bupropion outlines how we coordinate psychiatric and obstetric decision-making. Whole-person care also includes basic pregnancy health habits, from sleep and nutrition to checking products for safe ingredients for expecting mothers.
Making an Informed Decision with Your Provider
A common pregnancy visit goes like this. A patient tells us, "I want to do the safest thing for the baby, but I also need to keep my job, get to appointments on time, and not lose control of my day." That is usually where the true choice lies. The question is not whether medication risk exists in the abstract. The question is which plan creates the lowest overall risk for this specific pregnancy.
In practice, we build that decision around function, history, and monitoring. We want to know what happens when Vyvanse is reduced or stopped, what the pregnancy has looked like so far, and where the pressure points are at home and at work. A patient with mild symptoms, flexible routines, and strong support may do well with a taper. A patient with severe executive dysfunction, unsafe driving history, or repeated difficulty managing basic daily tasks may face more risk from symptom relapse than from staying on treatment with close follow-up.
Questions that actually change the plan
A useful appointment gets concrete quickly:
- How impaired are you without medication? We ask about driving, work performance, medication adherence, meal planning, finances, and keeping prenatal appointments.
- What is your obstetric and medical history? Blood pressure concerns, prior preterm birth, growth issues, hyperemesis, insomnia, and appetite problems all affect the plan.
- What support do you realistically have? A partner, family help, childcare coverage, and schedule flexibility can make a lower-dose or non-medication approach more realistic.
- What coexisting psychiatric symptoms are in the picture? Anxiety, depression, binge eating, trauma symptoms, and substance use history often matter as much as ADHD itself.
- What has happened in prior medication changes? If past stimulant tapers led to unsafe driving, job loss, or inability to manage basic routines, that history carries real weight.
We also discuss what each option requires. Continuing medication means more follow-up and clearer coordination with the obstetric team. Reducing or pausing medication means planning for the return of symptoms, not just hoping for the best.
What tends to go poorly
Three patterns create problems over and over.
- Stopping abruptly without a plan. Patients can feel exhausted, foggy, emotionally flat, and much less organized within days.
- Relying on generalized internet advice. Online discussions often mix prescribed use, misuse, and multiple different stimulants into one message.
- Treating psychiatry and obstetrics as separate conversations. Mixed recommendations leave patients stuck in the middle.
Our role is to help patients work through the trade-offs clearly. Sometimes that means continuing Vyvanse with monitoring. Sometimes it means lowering to the smallest dose that still preserves function. Sometimes it means building a structured fallback plan that uses sleep protection, therapy, environmental supports, and, in some cases, non-stimulant ADHD treatment options.
Whole-person care also includes the daily details that affect pregnancy tolerance. If a patient is simplifying routines and trying to reduce unnecessary exposures, practical resources on safe ingredients for expecting mothers can help with those non-psychiatric decisions too.
The best plan is individualized, documented, and revisited as the pregnancy changes. Symptoms change. Blood pressure changes. Work demands change. Good care leaves room to adjust.
Alternatives and Management Strategies During Pregnancy
A pregnancy ADHD plan has to work on real weekdays, not just on paper. If a patient cannot keep track of meals, appointments, driving safety, or medication instructions without treatment support, that matters. Our job at Integrative Psychiatry of America is to build a plan that protects both maternal functioning and pregnancy health, then adjust it as the pregnancy changes.
For some patients, the best option is to stay on Vyvanse with closer monitoring. For others, a dose reduction is reasonable. Others decide to taper off and replace medication support with a structured behavioral plan. The decision depends on how impairing the ADHD is, whether previous medication changes caused major decline, and what other pregnancy risk factors are present.
Comparing ADHD Management Options in Pregnancy
| Strategy | Description | Key Considerations for Pregnancy |
|---|---|---|
| Continue current stimulant with monitoring | Maintain Vyvanse when ADHD symptoms create meaningful safety or functioning problems without treatment | Often includes closer review of blood pressure, appetite, sleep, weight trends, and obstetric history |
| Reduce to the lowest effective dose | Preserve some symptom control while trying to lower medication exposure | Best suited to patients who can function adequately on less medication |
| Taper off stimulant gradually | Step down over time instead of stopping all at once | Gives the patient and care team time to track fatigue, mood, eating patterns, and executive function |
| CBT for ADHD | Builds routines, task breakdown, planning skills, and cognitive restructuring | Safe in pregnancy and often helpful for overwhelm, procrastination, and follow-through |
| ADHD coaching and environmental supports | Uses reminders, visual cues, accountability, simplified systems, and household structure | Works best when tools are concrete, repeated, and shared with partners or family when appropriate |
| Mindfulness, sleep hygiene, and nutrition support | Improves attention indirectly by reducing sleep disruption and stress load | Helpful as add-on support, but often not enough alone for moderate to severe ADHD |
| Non-stimulant evaluation | Reviews whether another medication approach fits the clinical picture | Requires individualized psychiatric review, not an automatic medication swap |
What helps most is specificity. "Try to stay organized" is rarely useful. Written morning checklists, shared digital calendars, automatic bill pay, meal repetition, landing spots for keys and medications, and body-doubling are more effective because they reduce executive load instead of asking the brain to push harder.
I often remind patients that medication changes expose the weak points in a routine very quickly. A patient who was barely keeping up before pregnancy may need more support, not less, after a stimulant reduction. That is why we usually build systems before symptoms spiral.
For patients who want to review options beyond stimulants, non-stimulant ADHD treatment approaches can be part of the discussion. These options are not automatically safer or easier in pregnancy. They still require a careful review of benefits, side effects, prior response, and the reason for making the switch.
Tapering works better when it is paired with replacement supports
A taper plan should answer practical questions. Who is helping with transportation if attention worsens? What happens if work performance drops? How will we respond if the patient develops marked fatigue, low mood, binge eating, or severe disorganization?
That planning matters just as much at home. If the patient is preparing for delivery while also trying to simplify feeding decisions for later, it can help to compare top newborn breast pumps early, alongside the rest of the postpartum setup.
A good pregnancy plan is rarely one intervention. It is a layered plan with medication decisions, therapy or coaching, home systems, partner involvement when available, and clear follow-up points for reassessment.
Navigating Postpartum Care and Breastfeeding on Vyvanse
The postpartum period often gets less planning than pregnancy, even though it can be the most destabilizing phase for ADHD. Sleep fragmentation, feeding schedules, hormonal shifts, and the constant demand for rapid task-switching can push symptoms into overdrive.

Guidance remains cautious because Vyvanse can pass into breast milk, and some consumer-oriented summaries note concerns such as irritability, poor feeding, or withdrawal-type symptoms in exposed infants. At the same time, a study summarized in the literature found no increase in neurodevelopmental disorders in children exposed prenatally to ADHD medications, as discussed in this review of prenatal ADHD medication outcomes.
What to monitor after delivery
Breastfeeding decisions need a practical plan, not just a yes-or-no label. If stimulant treatment continues postpartum, monitoring usually focuses on:
- Feeding: Watch for poor latch, weak intake, or unusual feeding difficulty.
- Behavior: Track irritability, agitation, unusual sleepiness, or trouble settling.
- Growth and pediatric follow-up: Keep routine infant checks and bring medication exposure into the conversation early.
- Maternal stability: Monitor whether untreated or undertreated ADHD is contributing to missed feeds, medication errors, dangerous fatigue, or mood decline.
Parents who are also sorting out pumping logistics may appreciate a practical guide to compare top newborn breast pumps while building a feeding plan that fits real life.
The fourth-trimester planning point
Postpartum psychiatric care should account for both infant exposure and maternal functioning. A mother who cannot organize feeds, sleep at all between wake-ups, or follow through on her own medical care may need a different plan than she expected during pregnancy.
This overview may also help frame the discussion with family and pediatric support:
The postpartum question isn't only whether Vyvanse enters milk. It's whether mother and baby are both functioning well on the actual plan being used at home.
How to Get Expert Support for Your Pregnancy Journey
Pregnancy and postpartum ADHD care works best when someone is actively coordinating the moving parts. That usually means psychiatric review of symptom severity, obstetric input on blood pressure and fetal growth, and a postpartum plan that includes feeding decisions and infant monitoring.
For patients who are building a wider preparation checklist, it can help to get ready for your journey to parenthood with practical planning outside the medication question too. The goal isn't perfection. It's reducing chaos before the baby arrives.
When urgent medical attention is needed
Seek urgent evaluation right away if the pregnant patient develops concerning symptoms such as severe headache, marked blood pressure concerns already identified by her medical team, chest pain, shortness of breath, heavy bleeding, or a sudden major change in fetal movement. For a newborn, urgent pediatric guidance is appropriate if there is poor feeding, unusual lethargy, significant irritability, trouble waking, or breathing concerns.
For ongoing psychiatric follow-up, online ADHD medication management can make treatment adjustments and check-ins easier to maintain during pregnancy and after delivery. Telepsychiatry can be especially useful when appointments need to happen from home with limited energy, transportation, or childcare.
A careful vyvanse pregnancy plan should answer four questions clearly. Should medication continue, taper, or change. What monitoring is needed during pregnancy. What is the feeding plan after delivery. And who should the patient contact if symptoms shift quickly.
If you're pregnant, planning pregnancy, or newly postpartum and trying to decide what to do about ADHD treatment, Integrative Psychiatry of America offers telepsychiatry for adults across Pennsylvania. A psychiatric nurse practitioner can review current symptoms, discuss medication trade-offs, coordinate with your OB clinician, and help build a treatment plan that fits pregnancy, recovery, and daily functioning.

