Typing “depression therapy Philadelphia” into a search bar often happens late. Maybe after another hard morning of getting out of bed, another workday pushed through on autopilot, or another evening of telling family and friends “I'm just tired” when that isn't the full truth.
That search can feel small, but it's a real step. Depression can make even basic decisions feel heavy, and starting care is often hardest before the first appointment is ever booked. In Philadelphia, that struggle isn't unusual. About 20% of adults in Philadelphia have been diagnosed with depression, and 19.3% of adults in Pennsylvania reported depression in 2023 according to Pennsylvania depression statistics.
Depression also doesn't always look the same from person to person. For some adults, it shows up as sadness and hopelessness. For others, it looks more like irritability, brain fog, low motivation, sleep disruption, or a sense that life has narrowed. Hormonal change can complicate the picture too, especially in midlife, which is why some readers may also find Lila's guide to perimenopause mood useful when mood symptoms seem tied to cycle changes or shifting hormones.
Philadelphia patients usually don't need more vague advice. They need a clear plan. This guide explains what depression treatment involves, how to compare therapy and medication options, how telehealth fits into modern care, and how to choose a provider with confidence. Adults who aren't sure whether symptoms have crossed the line into something that needs professional evaluation can also review when to see a mental health prescriber for depression symptoms.
Table of Contents
- Taking the First Step Toward Healing in Philadelphia
- What Depression Therapy Actually Involves
- Evidence-Based Depression Treatments We Use
- Telehealth vs In-Person Therapy A Modern Choice
- How to Choose the Right Provider in Philadelphia
- Your First Visits What to Expect and How We Track Progress
- Begin Your Journey to Wellness Today
Taking the First Step Toward Healing in Philadelphia
Starting depression treatment usually begins before any medication decision or therapy session. It starts with recognizing that something isn't working and that trying to push through alone hasn't fixed it. For many adults in Philadelphia, the hardest part is not treatment itself. It's narrowing down what kind of help is needed.
A useful first question is simple. Is the current problem mainly emotional pain, loss of functioning, or both? If someone still gets through work and daily responsibilities but feels persistently flat, hopeless, anxious, or disconnected, outpatient care is often the right place to start. If daily life is falling apart, symptoms are intensifying quickly, or safety is a concern, a higher level of care may be necessary.
A practical way to begin
A focused starting process helps reduce overwhelm:
- Name the main symptoms: low mood, loss of interest, sleep changes, guilt, fatigue, poor concentration, agitation, or numbness.
- Write down how long they've been present: not for a provider's convenience, but because timing shapes diagnosis and treatment choices.
- Notice patterns: some people worsen in the morning, some after social stress, some during hormonal shifts, and some with isolation or alcohol use.
- Decide what kind of first appointment is needed: therapy, medication evaluation, or a provider who can assess both.
Practical rule: If someone doesn't know whether therapy alone is enough, booking with a clinician who can evaluate both psychotherapy needs and medication options often saves time.
Philadelphia patients also face a real logistics problem. Search results often bounce between hospital pages, large directories, and private practices that sound similar on the surface. That's why choosing care works better when the search is narrowed by need, not by marketing language. “I need evening virtual appointments,” “I want medication and therapy discussion,” or “I need someone comfortable treating depression with anxiety and trauma history” are better filters than just searching for the nearest office.
What tends to help early
Early momentum matters. Patients are more likely to follow through when the first step is manageable.
Helpful first moves often include:
- Choosing one provider list, not five: insurance directory, referral from a primary care office, or one trusted practice website.
- Prioritizing availability: the best clinician on paper won't help if the first opening is too far out and symptoms are active now.
- Preferring clarity over prestige: a provider who explains process, follow-up, and fit is often more useful than one with a polished profile and little practical information.
What Depression Therapy Actually Involves
Therapy isn't passive venting. Good depression therapy is structured, collaborative, and aimed at change. Patients often come in worried they'll be asked, week after week, “How did that make you feel?” without any direction. That isn't the standard to look for.
A better way to think about therapy is this. It functions like skill-building with clinical guidance. The provider helps identify patterns that keep depression going, then works with the patient to interrupt those patterns through specific tools, new behaviors, and consistent review.
What happens in real sessions
In effective outpatient treatment, sessions often focus on a few concrete tasks:
- Spotting patterns: harsh self-talk, withdrawal, avoidance, perfectionism, or rumination.
- Testing behavior changes: sleep structure, activity scheduling, communication changes, or reducing avoidance.
- Building emotional range: learning how to tolerate sadness, shame, stress, and uncertainty without shutting down.
- Improving function: not just “feeling better,” but getting back to work, relationships, self-care, and purpose.
The therapeutic relationship matters, but fit alone isn't enough. A warm provider who never challenges stuck patterns may feel comforting without moving treatment forward. On the other hand, a highly technical provider who feels cold may lose trust before treatment has a chance to work.
Therapy should feel supportive, but it should also feel active. If sessions never translate into daily life changes, something needs to be adjusted.
What patients should expect from a good provider
A strong therapist or psychiatric nurse practitioner usually does several things well. They listen carefully, but they also organize what they hear. They don't treat every bad week as a treatment failure. They also don't let months pass without checking whether the current plan is helping.
Patients who want a general orientation to psychotherapy can review NAMI's overview of psychotherapy. It's a useful starting point for understanding how talk therapy fits into depression care.
A helpful question for any first consultation is: “How do you know if treatment is working?” The answer should be specific. It might involve symptom check-ins, goal review, sleep tracking, functioning at work, or changes in motivation and hopelessness. If the answer is vague, that's worth noticing.
Evidence-Based Depression Treatments We Use
Depression treatment works best when it matches the person in front of the clinician. Some adults need psychotherapy as the main intervention. Some need medication support to reduce symptom intensity enough to engage in therapy. Others benefit most from a combined model that addresses thoughts, behaviors, biology, and daily habits at the same time.
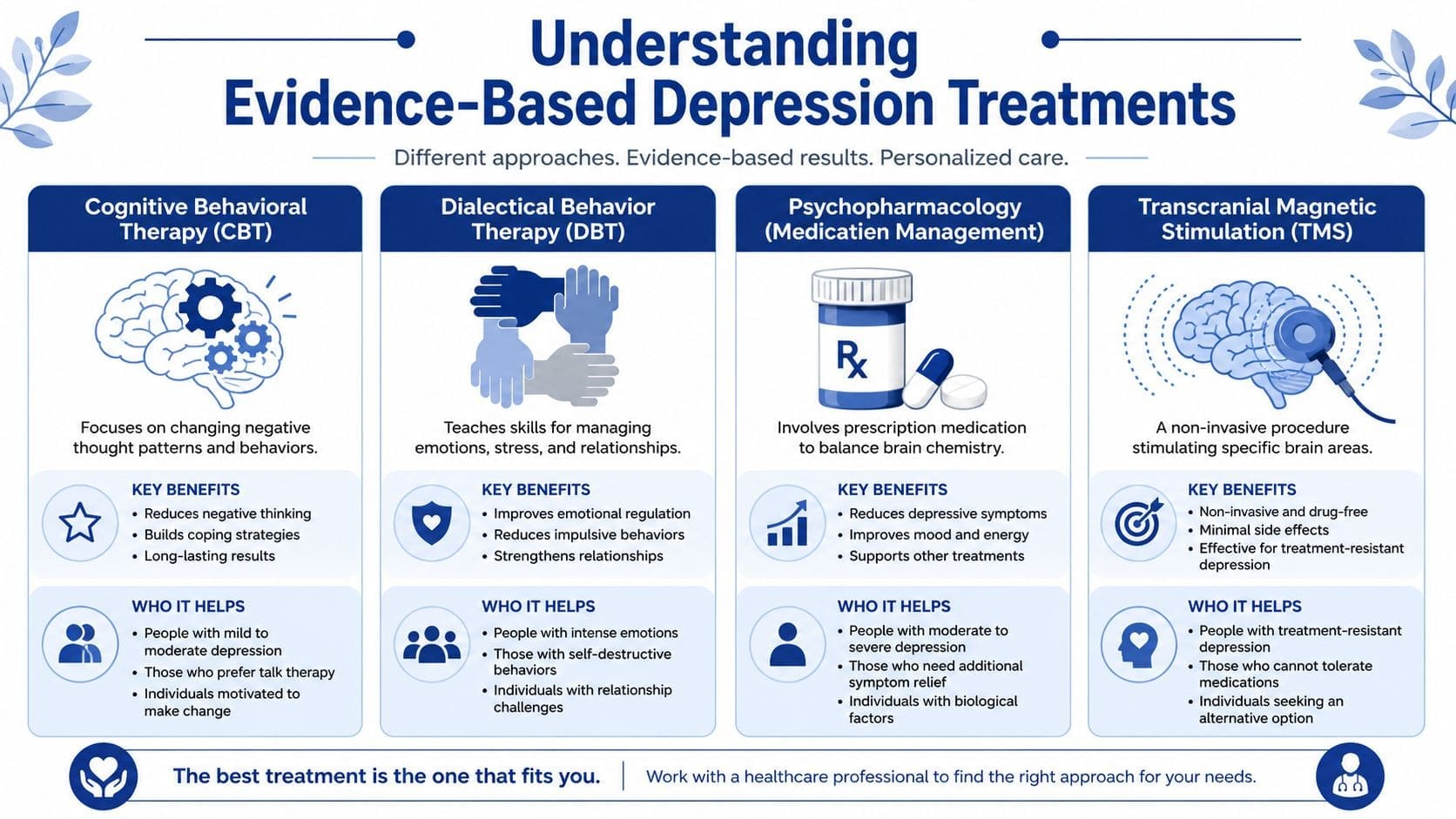
CBT, DBT, and medication management
Cognitive Behavioral Therapy or CBT is often a strong fit for depression that includes negative thinking, avoidance, hopeless predictions, and reduced activity. CBT helps patients notice distorted thoughts, challenge unhelpful assumptions, and reconnect behavior to mood improvement. It's practical and often appeals to adults who want concrete homework and a clear framework.
Dialectical Behavior Therapy or DBT can help when depression is mixed with emotional intensity, impulsive behavior, self-criticism, conflict in relationships, or difficulty tolerating distress. DBT teaches skills rather than relying only on insight. Patients often learn emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Medication management is not a shortcut and it isn't a replacement for psychological work. For some patients, though, medication can reduce depressive burden enough to make therapy more usable. That matters when symptoms include marked hopelessness, poor concentration, agitation, appetite disruption, or sleep problems that interfere with daily functioning.
A psychiatric nurse practitioner can assess these options together rather than forcing patients to split care immediately between multiple offices. One option available in Pennsylvania is Integrative Psychiatry of America's exercise-informed depression care resource, which reflects a model that combines psychiatric treatment with lifestyle interventions when clinically appropriate.
Why combined care often works better
Outpatient evidence relevant to Philadelphia care models shows that depression treatment often works best when it combines cognitive behavioral therapy, medication management, exercise, nutrition, and other behavioral therapies rather than relying on one approach alone, as described in Recovery.com's overview of depression treatment options in Philadelphia.
That matters because depression rarely stays in one lane. It affects sleep, energy, concentration, motivation, physical activity, appetite, and daily structure. A treatment plan that ignores those areas can miss major drivers of ongoing symptoms.
A brief comparison can help:
| Approach | Best use | Limitation if used alone |
|---|---|---|
| CBT | Negative thinking, avoidance, low motivation | May be harder to use when symptoms are severe |
| DBT | Emotional dysregulation, stress, relationship strain | Doesn't always address biological symptoms directly |
| Medication management | Moderate to severe symptom burden, sleep or concentration issues | Doesn't teach coping skills by itself |
| Exercise and nutrition support | Energy, routine, whole-person recovery | Usually not enough as a sole treatment for significant depression |
The most effective plan is usually the one a patient can actually follow consistently. A perfect plan on paper isn't useful if it doesn't fit energy, schedule, or symptom severity.
Telehealth vs In-Person Therapy A Modern Choice
Many Philadelphia adults don't need to choose between “serious care” and “convenient care.” Modern depression treatment can happen in either setting, and the better option often depends on symptoms, schedule, privacy needs, and how a patient functions best.
A visual side-by-side comparison can make that decision easier.
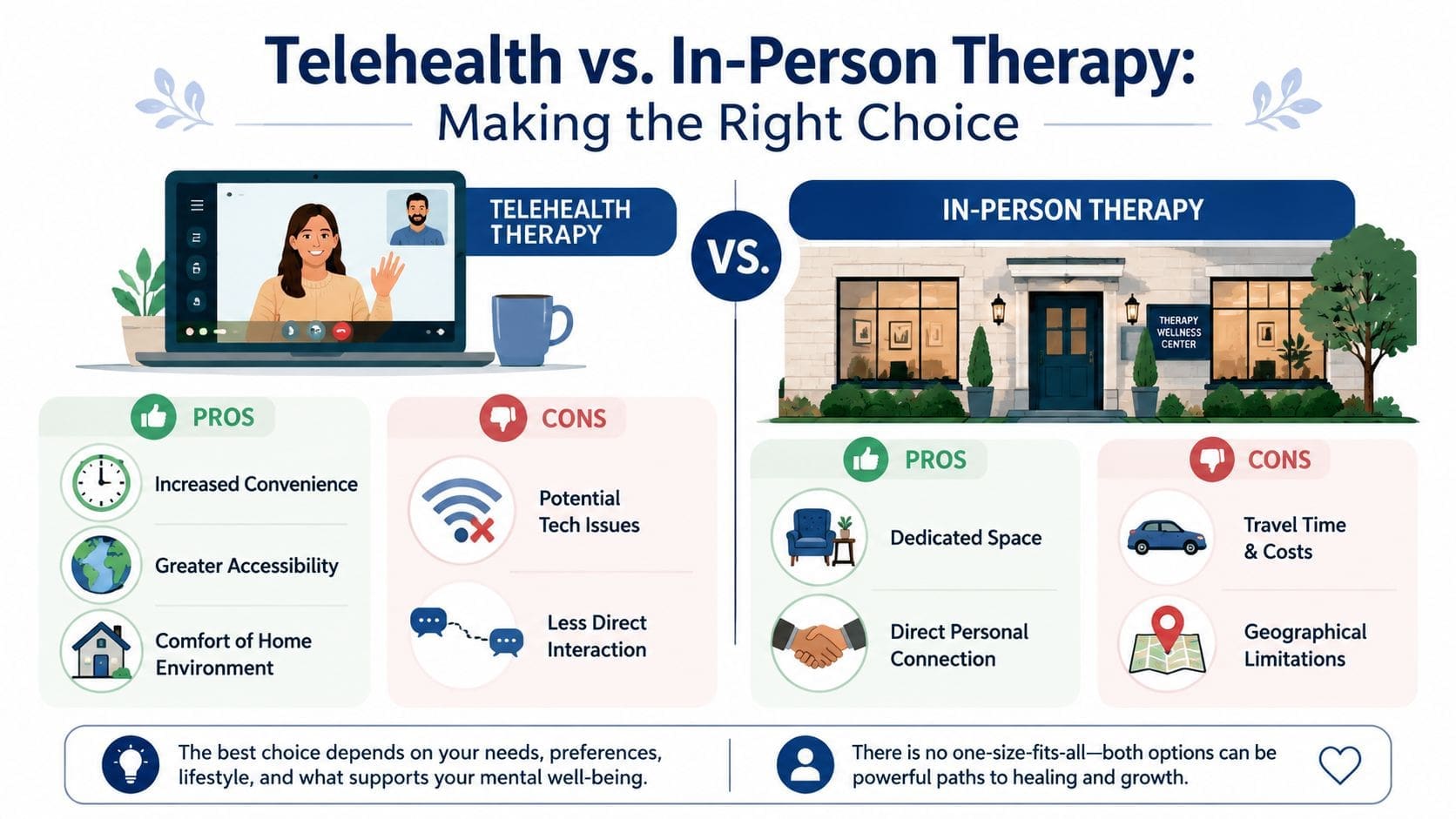
When telehealth fits well
Telehealth is often a strong match for adults who are depressed and low on activation. If getting dressed, commuting, parking, and sitting in a waiting room already feels like too much, removing those steps can make treatment more accessible. It also helps people with demanding jobs, caregiving responsibilities, limited transportation, or concerns about privacy in a dense city environment.
Telehealth can be especially useful for:
- Busy professionals: less disruption to the workday.
- Parents and caregivers: fewer childcare and travel complications.
- Patients who feel safer at home: some people open up more easily in a familiar space.
- Adults seeking medication follow-up: virtual check-ins can be efficient and clinically appropriate.
Patients considering virtual care can review online psychiatry for depression in Philadelphia to see how a telehealth-first model typically works.
A short overview may also help set expectations before the first appointment:
When in-person may be the better fit
In-person care still has value. Some patients concentrate better in a dedicated office. Some feel more contained and less distracted outside the home. Others prefer face-to-face presence, especially if they've struggled to connect through screens in other parts of life.
The right question isn't “Which is better?” It's “Which format makes it more likely that treatment will be attended consistently and used well?” For many adults with depression, consistency matters more than the setting itself.
How to Choose the Right Provider in Philadelphia
Finding the right provider takes more than reading a short bio and checking whether someone “treats depression.” Philadelphia patients often search for a psychiatrist, therapist, counselor, or medication prescriber without knowing how those roles differ in practice. That uncertainty can slow down care.
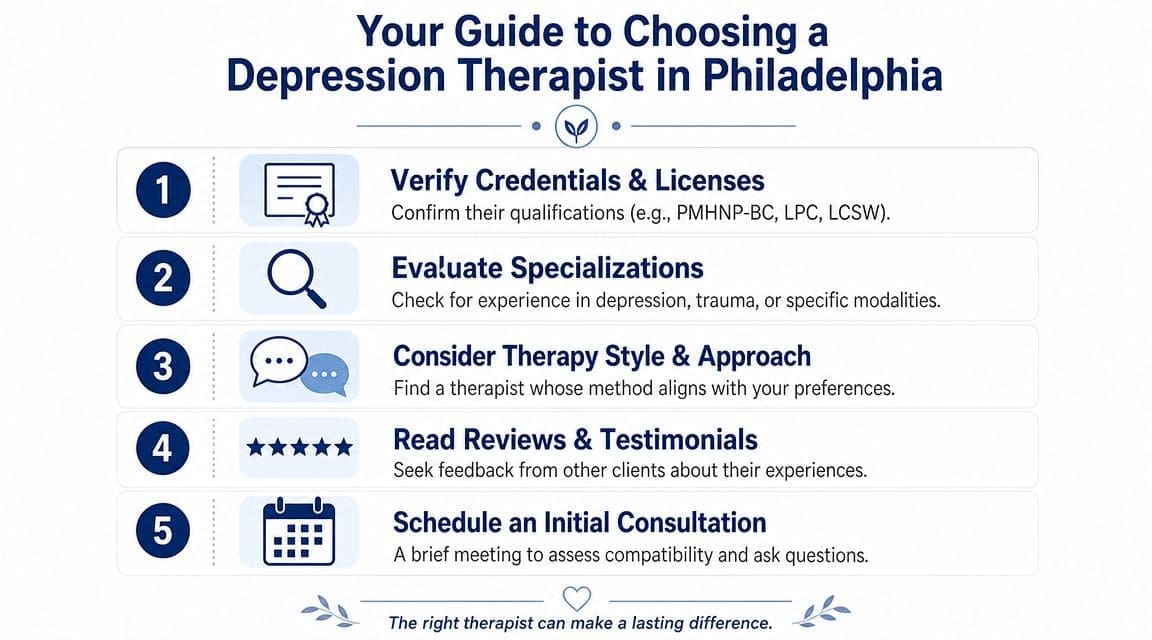
Credentials and scope of care
A provider's license matters because it shapes what they can evaluate and treat. Therapists such as LPCs and LCSWs provide psychotherapy. Psychiatric prescribers, including board-certified psychiatric nurse practitioners, can evaluate symptoms, diagnose mental health conditions, prescribe medication when indicated, and in many settings also provide supportive or structured therapeutic care.
Patients often search broadly for “psychiatrist” when what they really need is someone who can assess medication and therapy needs together. A useful explainer on that distinction is psychiatric NP vs psychiatrist.
Before booking, it helps to verify licensure directly through the Pennsylvania licensing verification system. That step sounds formal, but it's simple and worth doing.
Questions worth asking before booking
A brief consultation call or intake email should answer practical concerns, not just availability. Good questions include:
- What kinds of depression do they treat most often? Persistent low mood, postpartum concerns, trauma-related depression, bipolar depression, and depression with anxiety can require different approaches.
- Do they offer therapy, medication management, or both? This determines whether care will be coordinated or split across providers.
- How do they reassess treatment if symptoms don't improve? Strong providers have a clear follow-up process.
- What's their stance on telehealth vs in-person? Not every patient wants the same format.
- How often are visits scheduled early on? Patients should know what follow-up usually looks like.
A good fit isn't only about feeling comfortable. It's also about whether the provider can explain a method, monitor response, and adjust the plan when needed.
Cost insurance and access
Cost uncertainty is a major barrier in Philadelphia. One local provider cited by community reporting notes that sessions can range from about $130 to $160, and sliding-scale availability is often limited, according to The Philadelphia Citizen's guide to mental health services. That's why patients should ask about fees, insurance participation, cancellation policies, and refill or follow-up processes before the first visit, not after.
A practical checklist helps:
| What to ask | Why it matters |
|---|---|
| Do you take my insurance? | Avoids surprise billing |
| What is the self-pay rate? | Helps compare total cost clearly |
| Is there a waitlist? | Delays can matter when symptoms are active |
| Do you offer telehealth? | Expands scheduling flexibility |
| If I need more support, what happens next? | Shows whether the provider can triage appropriately |
Many patients also benefit from asking whether the practice helps determine level of care. Weekly outpatient therapy is appropriate for many people, but not everyone. Some adults need medication follow-up sooner. Some need group support. Some need more structured treatment than standard weekly visits.
Your First Visits What to Expect and How We Track Progress
The first few appointments shouldn't feel like guesswork. Good depression care starts with a thorough intake, a working formulation of what's driving symptoms, and a plan that can be observed over time instead of left vague.

What happens at intake
An intake usually covers current symptoms, psychiatric history, medication history, sleep, appetite, substance use, trauma exposure, medical factors, family history, and current life stress. Patients sometimes worry they need to tell their entire life story in perfect order. They don't. The clinician's job is to organize the information, ask follow-up questions, and identify what matters most right now.
The first visit often leads to one of several outcomes:
- Therapy-first plan: useful when symptoms appear manageable without medication at the outset.
- Medication evaluation with therapy support: helpful when symptom intensity is interfering with function.
- Combined treatment plan: often appropriate when both biological and behavioral symptoms are active.
- Recommendation for additional assessment: when diagnosis is unclear or medical contributors need review.
Patients interested in whether biology may affect treatment response sometimes also ask about genetic testing in depression care. It isn't a universal starting point, but it can be part of a broader evaluation in selected cases.
How progress gets measured
Depression treatment should be monitored, not just discussed. In structured psychotherapy research, a 50.0% reduction in IDS-SR symptoms by week 6 and 54.3% by week 8 predicted remission in combined treatment, while psychotherapy-only patients were identified more reliably at week 8, according to the measurement-based care study on depression remission prediction.
The practical takeaway is straightforward. Providers shouldn't wait until the end of treatment to decide whether it's helping. If symptoms aren't moving in the right direction, the plan may need to be adjusted earlier. That might mean changing therapy focus, reviewing diagnosis, revisiting medication strategy, or increasing support.
Early improvement isn't the only sign of success, but treatment should show direction. If there's no meaningful movement, reassessment is part of good care.
Begin Your Journey to Wellness Today
Depression is treatable, and finding care in Philadelphia doesn't have to stay confusing. The right starting point is usually the one that matches actual need, practical constraints, and the kind of support a person can consistently use. For some adults, that means weekly therapy. For others, it means therapy plus medication management, virtual visits, or a broader integrative plan.
People who want extra self-management tools alongside formal care may also appreciate this resource on unmedicated anxiety solutions, especially when stress and anxious symptoms overlap with depression. The key is not waiting for symptoms to become unbearable before acting.
If depression has been making daily life feel smaller, slower, or harder to manage, the next step can be simple. Integrative Psychiatry of America offers confidential online psychiatric care across Pennsylvania, including Philadelphia, with evaluation, medication management, and integrative treatment planning that can be started from home.

