Early changes such as better sleep, appetite, or energy can show up in 1 to 2 weeks, but significant mood improvement from Zoloft usually takes 4 to 6 weeks, and the fuller effect often becomes clearer around 8 to 12 weeks. That gap can feel long when someone has just picked up a new prescription and is hoping for relief now.
For many adults starting sertraline, the first few days bring a mix of relief, doubt, and impatience. The bottle is on the kitchen counter. Questions start immediately. Is it working yet? Is this side effect normal? How long before Zoloft starts working if the main problem is anxiety, depression, panic, or obsessive thoughts?
A board-certified psychiatric nurse practitioner usually frames this as a treatment process, not a test of willpower. Zoloft is often very useful, but it isn't a fast-acting medication in the way people often hope. The brain starts responding before a person feels better, and that difference matters. Understanding the timeline helps people stay consistent, report the right changes, and avoid stopping too early.
This article explains what the waiting period usually looks like, what can influence it, when to call a clinician, and how whole-person habits can support progress from day one.
Table of Contents
- Starting Your Zoloft Journey The First Steps
- Understanding How Zoloft Actually Works in Your Brain
- The Zoloft Onset Timeline What to Expect Week by Week
- Factors That Influence How Quickly Zoloft Works
- When to Contact Your Clinician About Your Zoloft Treatment
- Enhancing Zolofts Effectiveness with Integrative Psychiatry
- Frequently Asked Questions About Starting Zoloft
Starting Your Zoloft Journey The First Steps
A common starting point looks like this. An adult finishes a telehealth visit, hears that sertraline may help with depression symptoms, anxiety symptoms, panic attacks, OCD symptoms, or PTSD symptoms, and then spends the evening searching how long before Zoloft starts working. Hope is there, but so is worry about side effects, daily dosing, and whether this SSRI medication will help.
That concern is reasonable. Starting any antidepressant can feel like entering a waiting room without a clock. A psychiatric nurse practitioner usually helps by translating the process into something more practical. The early phase isn't empty time. It's a monitoring phase where sleep changes, appetite shifts, energy, nausea, restlessness, and emotional patterns all give useful information about how the medication is landing.

The waiting period is active treatment
People often assume no mood lift means nothing is happening. That isn't how sertraline works. The body and brain are adjusting from the first doses forward, even when emotional relief hasn't shown up yet.
A helpful mindset is to track patterns instead of chasing a dramatic overnight change. Useful questions include:
- Sleep quality: Is it easier to fall asleep, stay asleep, or wake up feeling less drained?
- Morning energy: Is getting out of bed slightly less difficult?
- Appetite and routine: Are meals, hydration, and daily structure becoming more regular?
- Anxiety level: Are there fewer spikes, even if overall anxiety is still present?
Lifestyle support matters here, too. Food intake, hydration, caffeine, alcohol, movement, and stress load can all affect how the first weeks feel. Readers interested in the connection between food and mental health can learn more from this guide on how nutrition affects mental health.
Many patients do better when they stop asking, “Do I feel cured yet?” and start asking, “What has shifted, even a little, since last week?”
What helps at the start and what usually doesn’t
What helps is consistency. Taking sertraline at the same time each day, keeping follow-up appointments, and writing down side effects gives a clinician something concrete to work with.
What usually doesn't help is changing the dose without guidance, skipping doses because of one rough day, or deciding in the first week that the medication has failed. Zoloft treatment works best when expectations match the actual antidepressant timeline.
Understanding How Zoloft Actually Works in Your Brain
A common first-week question in my practice is, “If the medication is in my system, why don’t I feel better yet?” That question makes sense. Sertraline starts affecting serotonin signaling early, but symptom relief usually follows on a slower schedule.
Zoloft, also called sertraline, is an SSRI, or selective serotonin reuptake inhibitor. It blocks the serotonin transporter, often called SERT, so more serotonin stays available between nerve cells in brain circuits involved in mood, anxiety, sleep, and stress regulation.
That first chemical shift is only part of treatment.
The harder part for patients is the waiting. Increased serotonin availability does not mean the brain has already adjusted in a way that leads to steadier mood, less anxiety, or better daily functioning. Those benefits depend on downstream changes in how brain networks communicate over time.
Serotonin changes first. The brain adapts after that.
This delay is one of the most important expectation-setting points when starting sertraline. Early in treatment, some people notice physical or behavioral changes before they notice emotional relief. Sleep may begin to settle. Panic may feel a little less intense. Irritability may soften before sadness lifts.
Part of the reason is that antidepressant response involves more than serotonin levels alone. The brain also goes through slower adaptive changes tied to learning, stress recovery, and neural flexibility. In plain language, sertraline helps create better conditions for healthier signaling patterns, but those patterns still need time to strengthen.
A related term you may see is 5-HT, which is another name for serotonin. This overview of what 5-HT means in psychiatry explains why serotonin matters in mood and anxiety treatment.
Medication works best when the whole nervous system gets support
Psychiatric nurse practitioners often take a broader view than medication alone. Sertraline can help, but the day-to-day environment you give your brain also matters. Poor sleep, heavy alcohol use, dehydration, high caffeine intake, constant stress, and inconsistent meals can amplify side effects or make it harder to notice early gains.
I tell patients to treat the first few weeks as a combined treatment phase, not a medication-only phase. Regular sleep, steady meals, movement, therapy, and nervous system regulation practices such as breathing exercises or mindfulness can support the same recovery process the medication is trying to promote. At IPA, that whole-person approach is part of the plan from day one.
What clinicians watch for early on
We do not just wait passively and hope for a dramatic change. We monitor for smaller signs that the medication is starting to fit. For anxiety, that may mean less physical tension, fewer spirals, or a shorter recovery time after stress. For depression, it may mean a little more motivation, improved concentration, or fewer barriers to basic tasks like showering, eating, or replying to people.
Those details matter. They help determine whether sertraline is beginning to help, whether side effects are settling as expected, and whether lifestyle or integrative supports need more attention while the medication takes hold.
The Zoloft Onset Timeline What to Expect Week by Week
You start sertraline on a Monday, then by Thursday you are asking the question nearly every new patient asks me. Should I feel something by now?
The honest answer is yes and no. Sertraline can cause effects in the first several days, but the effects patients want most, such as steadier mood, less anxiety, fewer intrusive thoughts, and a return of motivation, usually build more slowly. A practical timeline is this: early shifts may show up in the first 1 to 2 weeks, clearer symptom improvement often takes 4 to 6 weeks, and fuller benefit may continue developing over 6 to 8 weeks or longer, as summarized by HealthCentral on how long Zoloft takes to work.
That range matters because the first month often feels uneven. Some patients notice early relief. Some notice side effects first. Some feel very little at all until the dose has had enough time, or until sleep, therapy, nutrition, and stress regulation start supporting the same recovery process. At IPA, we plan for that full picture from day one rather than treating the medication as the only variable.
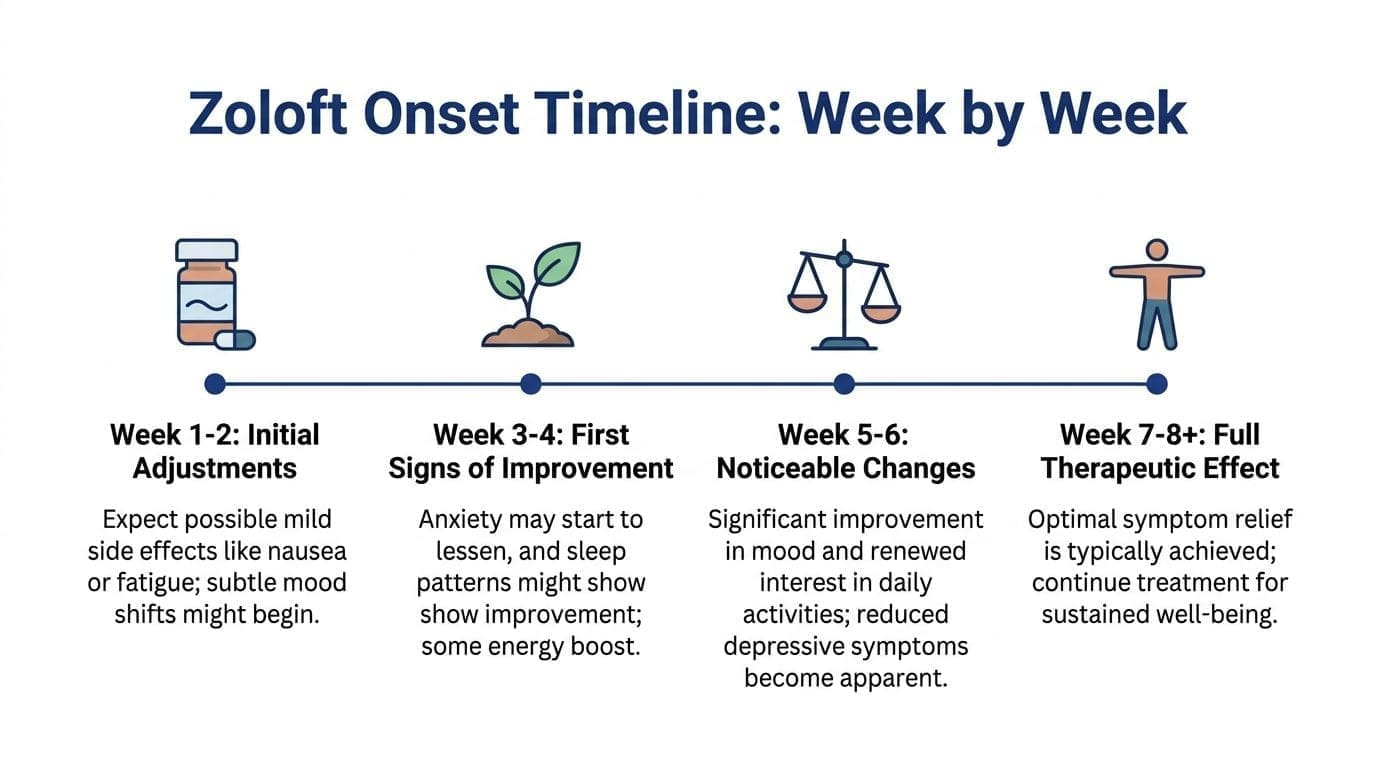
Weeks 1 to 2: adjustment first, benefit second
This phase is usually about tolerability.
Common early effects include nausea, looser stools, headache, reduced appetite, fatigue, trouble sleeping, or a keyed-up feeling. Those reactions do not automatically mean the medication is wrong for you. In many cases they soften over the next several days to two weeks.
Some patients also notice small positive changes early. Sleep may become more regular. Morning dread may ease slightly. Physical anxiety can feel less intense even if worries are still present. I tell patients to watch for reduced severity, not a complete disappearance of symptoms.
A few practical points help here. Take the medication at the same time each day. Stay hydrated. Keep caffeine and alcohol consistent or lower than usual, because big swings can make it harder to tell what is a medication effect and what is your nervous system reacting to lifestyle changes. If forgetfulness is part of the picture, this neurodivergent guide to medication adherence covers simple ways to make a daily routine more reliable.
Weeks 3 to 4: subtle gains become easier to spot
This is the point where improvement often becomes measurable in ordinary life.
You may still feel anxious or depressed, but the symptoms may have less force. Patients often report shorter spirals, less time spent crying, fewer panic surges, or an easier time getting through basic tasks. Family members sometimes notice the change first. You may sound more like yourself, answer texts, or stop canceling every plan.
This is also the stage where follow-up matters. If there is no benefit at all and side effects are persistent, the dose may need adjustment. If there is a small but real shift, staying the course is often reasonable. For some patients, especially those with a family history of medication sensitivity or multiple past medication failures, tools such as pharmacogenomic testing for depression medications can add useful context while the treatment plan is being refined.
Weeks 4 to 6: this is when many patients say, "I think it's helping"
By this stage, sertraline often becomes less about hope and more about evidence.
The evidence is usually functional. Work feels more manageable. The body is less stuck in fight-or-flight mode. Concentration improves enough to read, cook, drive, or complete a task without feeling overwhelmed. Depression may lift as a little more interest, energy, and emotional range. Anxiety may improve as less anticipatory fear and quicker recovery after stress.
The improvement can still be incomplete. That is common. A partial response at this point often leads to a thoughtful decision, not a snap judgment. Clinicians may continue the same dose a bit longer, increase gradually, strengthen therapy, or add targeted supports for sleep, exercise, trauma work, or nervous system regulation.
Weeks 8 to 12: fuller effect, or a decision point
Some conditions and some nervous systems need more time.
If sertraline is a good fit, benefits may continue to build across the second and third month. This is especially true when the start was slow, the dose was increased cautiously, or outside stressors were heavy during the first few weeks. Whole-person care matters here too. A patient who is sleeping five fragmented hours, drinking heavily on weekends, and skipping meals may have a much harder time noticing the true effect of the medication than a patient whose routine supports recovery.
By this point, I want patients looking at the whole trend. Are symptoms less intense, less frequent, or easier to recover from? Are daily responsibilities more manageable? Is there enough improvement to justify staying with the plan? Those are better questions than asking whether the medication created a dramatic emotional shift.
| Timeframe | What Patients May Notice | Common Side Effects That Often Improve |
|---|---|---|
| Week 1 to 2 | Early signs such as steadier sleep, slightly less physical anxiety, or improved appetite for some patients | Nausea, headache, fatigue, sleep disruption, feeling activated |
| Week 3 to 4 | More consistency in routines, fewer spirals, less avoidance, early functional improvement | Some startup effects may still linger but often begin easing |
| Week 4 to 6 | Clearer symptom relief in depression or anxiety, better daily functioning | Side effects are often milder if the medication is settling in well |
| Week 8 to 12 | Fuller therapeutic benefit, or enough information to reassess the plan | Ongoing side effects or minimal benefit should prompt a prescribing review |
Factors That Influence How Quickly Zoloft Works
I often tell new patients this at the start. The calendar matters, but the context matters too. Two people can take the same dose of sertraline and move at very different speeds because the diagnosis, the dosing plan, the body, and daily habits all affect what happens over the first several weeks.
The condition being treated changes the timeline
Sertraline does not show up the same way across diagnoses. In practice, panic symptoms may ease earlier than depression-related low motivation, and OCD often takes longer than either one. Patients with obsessive thoughts and compulsions usually need more time, and sometimes a higher target dose, before the benefit is clear.
That difference matters for expectations. A person taking Zoloft for panic may notice fewer body-based fear symptoms first. A person taking it for depression may notice that getting through the day feels less effortful before mood feels noticeably better. Good prescribing starts with matching the expected timeline to the actual condition being treated.
Dose, sensitivity, and metabolism all affect pace
The starting dose shapes the experience. Some patients begin at 50 mg. Others start lower because they are sensitive to nausea, activation, sleep disruption, or past side effects with SSRIs. That slower approach can make treatment easier to stay with, but it often means it takes longer to reach the dose that gives the full effect.
Metabolism matters too. Some people process sertraline more slowly and feel side effects more strongly without getting faster symptom relief. For patients who want to understand whether biology may be affecting tolerability or medication fit, this guide to depression genetic testing is a useful starting point.
Consistency matters more than many patients expect
One of the most common reasons the response looks unclear is inconsistent use. Missed doses, taking it at different times every day, or stopping and restarting can make side effects harder to interpret and benefits harder to track.
I pay close attention to this in patients with ADHD, autism, high anxiety, shift-work schedules, or a lot of family demands. If routine is hard to maintain, practical systems often help more than willpower alone. Patients who need that kind of structure may benefit from this neurodivergent guide to medication adherence.
Whole-person factors can either support or slow progress
Medication does not work in isolation. Poor sleep, alcohol use, appetite changes, chronic stress, inflammatory medical conditions, and drug interactions can all affect how a patient feels during the first month. Sometimes Zoloft is working, but the person is still running on four or five hours of broken sleep and cannot feel the gain clearly.
This is one reason psychiatric nurse practitioners look beyond the prescription pad. At IPA, we often pair medication treatment with sleep support, psychotherapy, nutrition guidance, nervous system regulation skills, and other integrative strategies from day one. That approach does not replace sertraline. It gives the medication a better chance to help.
A short visual explanation can also help clarify why response speed varies from person to person.
Variables that often affect the timeline
- Diagnosis: OCD, panic disorder, PTSD, and depression often improve on different schedules
- Dose plan: a cautious titration may improve tolerability but delay reaching a fully therapeutic dose
- Metabolism: liver enzyme differences can affect side effects and drug levels
- Consistency: missed doses or irregular timing can blur progress
- Other medications and health conditions: interactions or medical issues can change response and tolerability
- Lifestyle support: sleep, alcohol use, stress load, therapy, and daily routine can influence how much benefit a patient notices and how quickly
When to Contact Your Clinician About Your Zoloft Treatment
A common early treatment moment looks like this. You started Zoloft, it has been a couple of weeks, and now you are wondering whether the nausea, poor sleep, or lack of obvious improvement means something is wrong. In practice, that question is part of routine care. I want patients to reach out early enough to fix problems before they become reasons to quit a medication that may still help.
The main job here is to sort expected adjustment issues from problems that need fast medical attention. Mild side effects can often be managed with timing changes, dose adjustments, food intake, sleep support, or a slower titration. Safety concerns need same-day contact, urgent care, or emergency help.
Common issues that can usually be discussed at follow-up
Some concerns deserve attention soon, but they do not usually require the ER. A scheduled follow-up, portal message, or telehealth visit is often the right next step.
Contact your clinician about
- Side effects that keep hanging on: nausea, insomnia, fatigue, headaches, sexual side effects, or feeling emotionally flat without gradual improvement
- Unclear benefit after a fair trial: if you are taking it consistently and still not seeing meaningful change after several weeks, your dose, diagnosis, or treatment plan may need review
- Trouble taking it consistently: missed doses, uncertainty about the best time to take it, or stopping and restarting
- Daily functioning still slipping: work, parenting, school, relationships, or basic self-care still feel unmanageable
If symptoms are not improving after a reasonable trial, I reassess the full picture. That includes dose, side effects, sleep, substance use, therapy support, medical issues, and whether the original diagnosis still fits. At IPA, whole-person follow-up matters here because medication response can look weaker when anxiety is being fueled by insomnia, alcohol, poor nutrition, or constant stress load.
Signs that need prompt medical attention
Some symptoms should not wait for the next appointment.
Get urgent help right away for signs of an allergic reaction, possible serotonin toxicity, or a sudden mental health crisis.
Seek immediate care for
- Allergic reaction symptoms: swelling, trouble breathing, hives, or a fast-spreading rash
- Possible serotonin syndrome: confusion, agitation, heavy sweating, tremor, muscle stiffness or twitching, diarrhea, or rapid heartbeat
- Sharp worsening in mood or behavior: suicidal thoughts, self-harm urges, severe agitation, or behavior that feels markedly out of character
- Unsafe loss of functioning: not sleeping for long stretches, not eating, becoming disoriented, or being unable to care for yourself safely
Families and partners often notice these changes before the patient does. If someone close to you is worried, take that seriously.
Patients do not need to guess perfectly. If you are unsure whether a symptom is routine or urgent, contact your prescriber. If you are trying to decide whether your symptoms call for specialty psychiatric care, this guide on when to see a psychiatric provider can help. Some patients also benefit from added structure around sleep, stress, and body-based recovery habits through medically supervised wellness while medication treatment is being adjusted.
Enhancing Zolofts Effectiveness with Integrative Psychiatry
Medication can open a door, but it rarely does every part of the job by itself. Sertraline may improve serotonin signaling and support the brain changes discussed earlier, but daily habits still influence how recovery feels. Sleep debt, high alcohol use, poor nutrition, constant stress, and inactivity can all work against progress.
That doesn't mean people need a perfect lifestyle before starting treatment. It means whole-person care often gives medication a better environment to work in.

Medication works better when the rest of life supports recovery
Patients often underestimate how much friction daily life creates. If someone is sleeping erratically, eating once a day, skipping hydration, and white-knuckling through panic symptoms without coping tools, medication may still help, but the path can feel rougher.
Psychotherapy is one major support. For anxiety treatment and depression treatment, therapy can help patients challenge fear patterns, reduce avoidance, and build routines while waiting for medication effects to accumulate. That matters because medication doesn't teach coping skills. It creates more room to use them.
Recovery is easier to notice when symptoms are tracked alongside sleep, food, movement, stress, and therapy work, not just pill counts.
Whole person strategies that support treatment
A practical integrative plan usually includes a few core pieces rather than a long list of wellness tasks.
- Nutrition support: regular meals, protein intake, hydration, and reduced swings in caffeine or alcohol can make treatment easier to tolerate. This overview of SSRI supplements and diet for depression explores those foundations in more depth.
- Exercise counseling: consistent movement can help with energy, stress regulation, and daily structure. It doesn't need to be intense to be useful.
- Mindfulness and meditation: these practices can lower reactivity and help patients respond to anxious thoughts without getting pulled fully into them.
- Psychotherapy: CBT and other evidence-based approaches can reinforce the same recovery patterns medication is trying to support.
- Medical coordination: some people also benefit from broader health support when weight, sleep, hormones, or chronic stress are affecting psychiatric recovery. Resources on medically supervised wellness can be useful when care needs to extend beyond medication alone.
This approach is especially valuable in telehealth psychiatry, where adults across Pennsylvania may need practical treatment that fits real life in Philadelphia, the suburbs, small towns, or rural areas. Online psychiatry works best when the care plan includes both medication management and concrete daily supports.
Frequently Asked Questions About Starting Zoloft
Starting sertraline usually brings a handful of practical questions that don't always make it into the prescription discussion. These are some of the most common.
What should someone do if a dose is missed
The safest answer is to follow the prescribing instructions and contact the clinician or pharmacist if there’s any uncertainty. In general, people shouldn't double the next dose on their own. What matters most for Zoloft treatment is getting back to a consistent routine.
A missed dose here and there doesn't automatically mean the medication has failed. Repeated missed doses can make side effects and response harder to interpret.
Can someone drink alcohol while taking Zoloft
Many clinicians advise caution because alcohol can worsen depression symptoms, increase sedation for some people, disturb sleep, and make it harder to tell whether the medication is helping. It can also lower adherence. If alcohol use is regular or heavy, that deserves an honest conversation during medication management.
Will Zoloft change someone’s personality
The goal isn't to create a different person. The goal is to reduce symptoms that are getting in the way of functioning. When sertraline works well, people often say they feel more like themselves, not less. If someone feels emotionally flat, detached, or unlike themselves, that should be discussed with the prescriber.
How will someone know if it’s working
Improvement often shows up in daily function before it shows up in dramatic emotion. Signs may include better sleep, reduced dread, fewer crying spells, less avoidance, more patience, or greater ability to complete ordinary tasks.
Useful markers to watch
- Mood: less hopelessness or less frequent emotional crashes
- Anxiety: fewer panic surges, less rumination, or less physical tension
- Function: better concentration, self-care, work consistency, or social engagement
- Tolerance: side effects easing while benefits slowly build
How will someone know when it’s time to stop
That decision should be made with a licensed prescriber, not by stopping suddenly after a better week. The right timing depends on diagnosis, relapse history, how stable the person has been, and whether therapy and coping habits are in place. Stopping too early can make it hard to know whether the medication had a fair trial.
Does taking it longer mean it will definitely work
No medication works for everyone. Sertraline is a strong option for many adults, but if a person has little progress after a proper trial, the next step may be a dose change, another medication, or an added therapy approach. The key is assessment, not guessing.
If someone in Pennsylvania is looking for thoughtful telehealth medication management, therapy-informed care, and a whole-person plan for anxiety, depression, OCD, PTSD, ADHD, or related concerns, Integrative Psychiatry of America offers online psychiatric care designed to meet patients where they are.

