Some people start to wonder about this question after months of doing everything they were told to do for depression. They’re sleeping more, trying therapy, taking medication as prescribed, forcing themselves through work, and still waking up exhausted. Their body feels heavy. Their thinking feels slow. Their mood feels flat.
That pattern matters. Depression can absolutely cause low energy and brain fog, but it isn’t the only explanation. Sometimes the missing clue is physical, not purely psychological. One of the most overlooked examples is anemia, especially iron deficiency.
For a psychiatric nurse practitioner, this question isn’t theoretical. It comes up when someone says their mood treatment is only helping halfway, or when sadness is tangled up with weakness, dizziness, poor stamina, or feeling cold all the time. In those situations, asking can anemia cause depression is part of good psychiatric care, not a side issue. Mental health treatment works better when the body is evaluated with the same seriousness as the mind.

A whole-person assessment often changes the conversation. Someone who thought they were “just depressed” may be dealing with depression plus a treatable nutritional or hematologic problem. Someone who assumed they needed a stronger psychiatric medication may need lab work added to the plan. For people wondering when symptoms deserve a deeper evaluation, this guide on when to see a mental health prescriber is a useful starting point.
Table of Contents
- Introduction The Unseen Weight of Fatigue and Low Mood
- The Overlooked Connection Anemia and Your Mental Health
- How Anemia Fuels Depressive Symptoms The Biological Mechanisms
- Is It Depression Anemia or Both Untangling the Symptoms
- A Guide to Lab Testing for Mood and Energy
- Integrative Treatment Healing Mind and Body Together
- Your Next Steps for Comprehensive Care in Pennsylvania
- Frequently Asked Questions
Introduction The Unseen Weight of Fatigue and Low Mood
A common presentation in psychiatric practice looks like this. An adult says they feel depressed, but the word doesn’t seem big enough for what’s happening. They’re not just sad. They’re drained, unfocused, unmotivated, and physically worn down.
Sometimes they’ve already tried a reasonable depression plan. They may be in therapy. They may already be taking medication. Yet the fatigue keeps winning, and daily life starts to feel like pushing through wet cement.
That’s when the body has to be part of the workup. Can anemia cause depression? Yes, it can. It can also intensify depressive symptoms, mimic them, or sit beside them and make recovery feel frustratingly incomplete.
When low mood has a physical layer
Anemia means the body isn’t carrying oxygen as effectively as it should. Iron-deficiency anemia gets the most attention, but low vitamin B12 or folate can also contribute to an anemic picture and can affect mood, cognition, and energy in ways patients feel every day.
A mental health evaluation that ignores those basics can miss an important driver of symptoms. That’s one reason nutrition and physiology belong in psychiatric care. Readers interested in the broader relationship between food, deficiencies, and mood can learn more from this article on how nutrition affects mental health.
Low mood isn’t always “all in your head.” Sometimes the bloodwork changes the treatment plan more than another medication adjustment.
Why this question matters
People often blame themselves before they consider a medical contributor. They think they’re lazy, unmotivated, or failing treatment. In reality, a biologic issue may be reducing resilience from underneath them.
That doesn’t mean every depressed person has anemia. It does mean persistent fatigue, brain fog, poor concentration, weakness, or slow improvement deserve a wider lens.
The Overlooked Connection Anemia and Your Mental Health
The connection between anemia and depression is stronger than many people realize. This isn’t just a vague clinical suspicion. It’s a pattern that shows up in research and in real patient care.
What anemia actually means
Anemia is a condition in which the blood doesn’t adequately deliver oxygen to tissues. Iron deficiency is a common cause, but it isn’t the only one. Low B12 and low folate can also contribute, and each can bring its own mix of physical and cognitive symptoms.
For mental health, iron deficiency deserves special attention. Iron affects energy production, brain chemistry, and oxygen delivery. When it’s depleted, a person may look depressed, feel depressed, or become more vulnerable to depression.
Why mental health clinicians should care
The research is difficult to ignore. A 2023 meta-analysis examining twenty-six studies found that adults with iron-deficiency anemia were almost twice as likely to screen positive for major depressive disorder compared with iron-replete peers. The same review summarized NIH research showing that people with untreated anemia had a 2.6-fold increased odds of depression, with depression prevalence at 28.6% in untreated anemia compared with 14.4% in those without self-reported anemia, as described in this review of low iron and mental health findings.
That changes how a careful psychiatric assessment should work. If someone presents with depression plus pronounced fatigue, poor stamina, or cognitive slowing, anemia shouldn’t be treated like an unrelated primary care issue. It belongs in the differential.
Clinical takeaway: Depression treatment is less precise when fatigue, fogginess, and weakness are treated as purely emotional symptoms without checking for anemia.
A practical distinction also matters here. Untreated anemia carries the concern. Once anemia is properly treated, the depression risk picture looks different, which becomes important when discussing recovery and treatment planning later.
How Anemia Fuels Depressive Symptoms The Biological Mechanisms
A patient may tell me, “I’m sleeping enough, but I still feel flat, foggy, and exhausted.” In practice, that is a cue to look beyond a primary mood disorder and ask whether the brain and body have the materials they need to function well.

Iron is raw material for brain chemistry
Iron supports the production and regulation of monoamine neurotransmitters, including serotonin, dopamine, and norepinephrine. Those systems shape mood, motivation, concentration, reward, and stress tolerance. When iron is low, the brain can struggle to make and use these chemicals efficiently, which can look a lot like depression in day-to-day life.
Iron also matters for brain tissue itself. Earlier research discussed in this article describes effects on hippocampal function and neurogenesis, which helps explain why low iron can show up as low mood, mental slowing, and reduced resilience under stress.
This is one reason an integrative psychiatry approach matters. If treatment focuses only on antidepressant selection while ignoring iron deficiency, folate status, B12, sleep, and inflammation, the plan may be incomplete from the start.
Oxygen delivery affects how the brain feels and functions
Anemia also reduces oxygen delivery to tissues, including the brain. That does not always cause dramatic neurologic symptoms, but it often shows up as fatigue, weak stamina, headaches, poor exercise tolerance, and cognitive drag. Many patients describe it as feeling mentally dimmer or less able to recover from ordinary demands.
That physiologic strain can feed depressive symptoms in a very practical way. It is harder to stay engaged, active, hopeful, and emotionally steady when basic energy production is impaired.
Low ferritin can matter before anemia is obvious
Another clinical point gets missed often. A person can have depleted iron stores before hemoglobin falls far enough to trigger concern on a routine screen. In that stage, mood symptoms, brain fog, hair shedding, restless legs, or exercise intolerance may already be present.
That is why I encourage patients to ask what was tested, not just whether “iron” was checked. Hemoglobin alone does not tell the full story. Ferritin, iron indices, B12, folate, and sometimes related markers help clarify whether low mood has a biologic contributor that deserves treatment.
For people who also deal with attention problems, methylation concerns, or other biologic contributors to psychiatric symptoms, related nutrient pathways matter too. This explanation of methylfolate for MTHFR support is relevant because folate status can affect both brain function and blood health. During postpartum evaluation, the same principle applies, since fatigue and low mood can have overlapping medical and psychiatric drivers. Some patients also need support for postpartum challenges while iron status and other labs are being sorted out.
A short visual explanation can help make the physiology easier to grasp.
When iron is low, mood symptoms are not “just in your head.” The brain may be working with less support for neurotransmitter production, oxygen delivery, and stress regulation.
Is It Depression Anemia or Both Untangling the Symptoms
The hardest part for many adults is that depression and anemia can feel almost identical at first. Both can show up as fatigue, poor concentration, irritability, and loss of momentum.
Where the symptoms blur
A person with depression may say, “Nothing sounds enjoyable anymore.” A person with anemia may say, “Everything feels like too much effort.” Someone with both may struggle to tell where one ends and the other begins.
That overlap is especially relevant during major life transitions. For example, new parents dealing with exhaustion and emotional strain may benefit from reading about support for postpartum challenges, since postpartum mood symptoms can be complex and deserve careful evaluation.
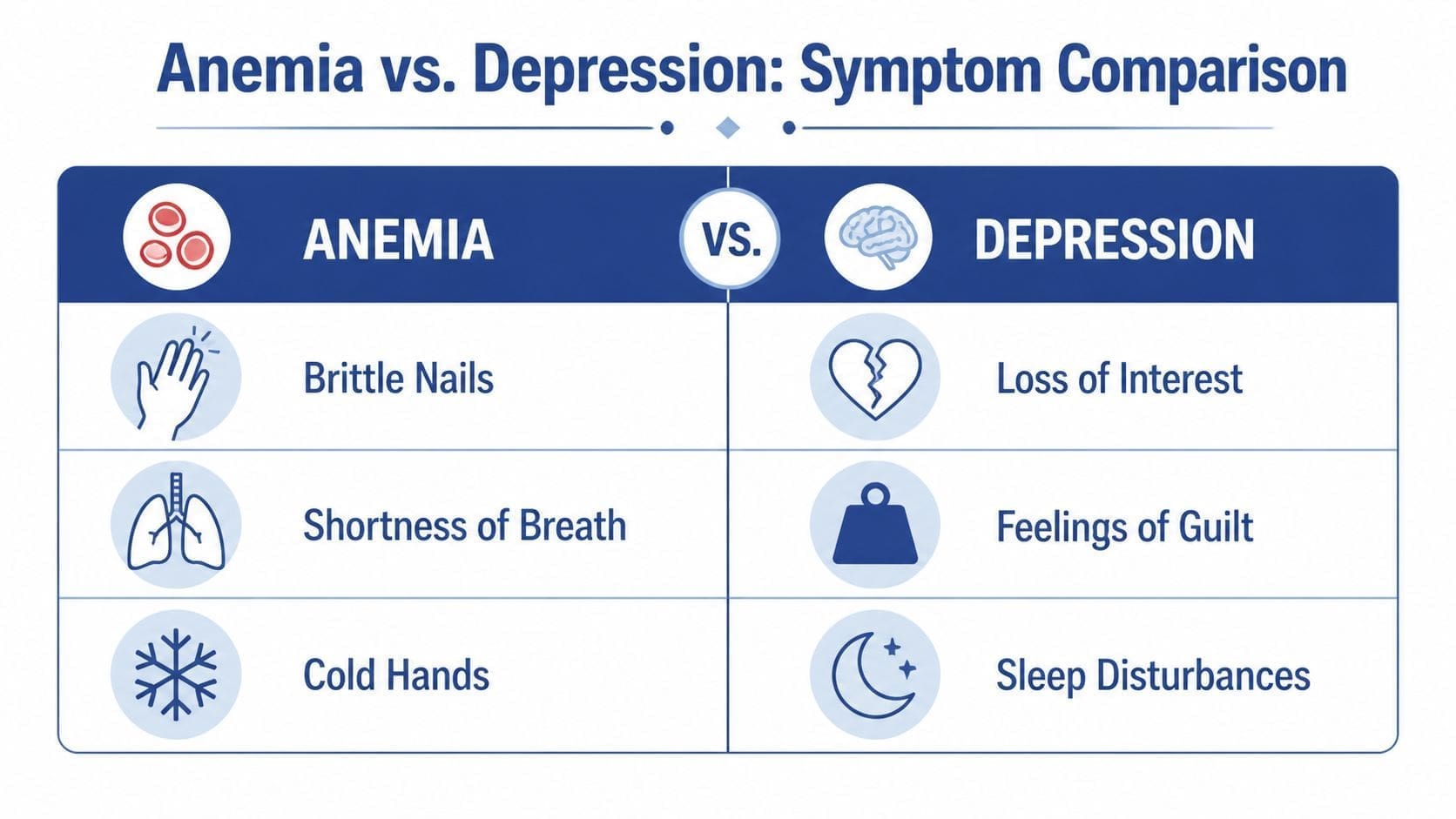
Symptom Overlap Depression vs. Anemia
| Symptom | Primarily Depression | Primarily Anemia | Common Overlap |
|---|---|---|---|
| Persistent sadness | Yes | Sometimes indirectly | Can occur |
| Loss of interest or pleasure | Yes | Less typical | Can coexist |
| Feelings of guilt or worthlessness | Yes | No | Less common overlap |
| Pale skin | No | Yes | No |
| Shortness of breath with exertion | No | Yes | Sometimes confused with low motivation |
| Cold hands and feet | No | Yes | No |
| Brittle nails | No | Yes | No |
| Profound fatigue | Sometimes | Yes | Yes |
| Difficulty concentrating | Yes | Yes | Yes |
| Irritability | Yes | Yes | Yes |
| Low motivation | Yes | Yes | Yes |
| Sleep disturbance | Yes | Sometimes | Yes |
| Physical weakness | Less typical | Yes | Yes |
A table like this doesn’t diagnose anything. It helps people ask better questions. If fatigue is paired with pale skin, shortness of breath, dizziness, brittle nails, or feeling unusually cold, that’s a clue to request lab testing instead of assuming the entire problem is psychiatric.
A Guide to Lab Testing for Mood and Energy
When someone asks can anemia cause depression, the next practical question is what to test. Clarity is essential, because a generic “labs were normal” doesn’t always settle the issue.
The labs worth discussing
A useful starting panel often includes:
- Complete Blood Count or CBC. This looks at red blood cells, hemoglobin, and hematocrit. It helps identify whether anemia is present.
- Serum ferritin. Ferritin reflects stored iron. This is often the key test when mood symptoms, fatigue, and brain fog show up before obvious anemia.
- Iron studies. A fuller iron panel can include serum iron, iron saturation, and total iron binding capacity. It gives context that ferritin alone can’t always provide.
- Vitamin B12. Low B12 can affect energy, cognition, and mood.
- Folate. Folate matters for both blood formation and nervous system function.
People with focus problems or long-standing fatigue sometimes discover that iron biology has been ignored for years. This article on ADHD and iron deficiency is helpful for understanding that crossover.
Why a basic check can miss the real issue
A common problem is stopping at one reassuring number. Hemoglobin might still sit inside a lab range while iron stores are running low. That’s one reason ferritin deserves direct attention in a mood and energy workup.
Ask what was actually tested, not just whether “iron” was checked.
Another practical point is interpretation. A primary care clinician, psychiatric nurse practitioner, or other prescriber may all order these labs, but the essential value comes from connecting the results to symptoms. That’s how subtle deficiencies stop being dismissed as stress, burnout, or lack of willpower.
Integrative Treatment Healing Mind and Body Together
A patient starts an antidepressant, gives it a fair trial, and still says, “I’m sleeping enough, but I feel drained and flat all day.” That is the point where I stop treating mood symptoms in isolation. If anemia, iron deficiency, or another nutrient problem is contributing, the plan has to address the biology as well as the depression.
Treatment is more precise once a cause is identified. Low iron stores, iron deficiency anemia, B12 deficiency, folate deficiency, blood loss, inflammation, and absorption problems do not call for the same response. Psychiatric medication may still help, but it often works better when the body has what it needs to make energy, carry oxygen, and support brain function.
Matching treatment to the cause
Oral iron is often the first step because it is accessible and familiar. It can work well for mild deficiency and for patients who tolerate it. The trade-off is adherence. Constipation, nausea, stomach pain, and poor absorption are common reasons people stop early or never reach a meaningful improvement.
IV iron is a stronger option in the right setting. It usually makes more sense when oral iron is not tolerated, iron stores remain low despite treatment, symptoms are persistent, or blood loss is ongoing. It requires more coordination and is not necessary for every patient, but it can be the more realistic choice when the goal is to restore function instead of waiting months for partial improvement.
The same principle applies beyond iron. B12 deficiency may need oral replacement or injections. Heavy menstrual bleeding may need gynecologic evaluation. Gastrointestinal blood loss may call for primary care or GI follow-up. If the cause is never treated, the mood plan stays incomplete.
What integrative psychiatric care looks like in practice
In an integrative psychiatry model, lab findings are not treated as a side note. They change the treatment plan. That may mean adjusting medication expectations, correcting deficiencies, coordinating with primary care, reviewing nutrition, and watching whether energy, focus, motivation, and mood improve as the underlying problem improves.
Therapy still matters. Sleep still matters. Medication still matters.
But if someone is iron deficient, asking them to push through exhaustion with willpower, coping skills, and a medication change alone is not good care. The work is to treat the depressive symptoms and the physiologic drivers at the same time.
For Pennsylvania patients who want remote psychiatric care that includes medication management and review of relevant labs when appropriate, this page on online depression treatment in Pennsylvania explains what that process can involve.
Some readers also want a broader view of non-medication support alongside medical treatment. The Axelrad Clinic's depression insights offer another useful perspective on integrative depression care.
Your Next Steps for Comprehensive Care in Pennsylvania
If depression treatment hasn’t fully helped, and fatigue still feels disproportionate, it’s reasonable to ask for a broader evaluation. That’s especially true when low mood is mixed with weakness, dizziness, poor exercise tolerance, brain fog, or other physical symptoms.
The next step is simple. Bring the full picture to a qualified clinician. Don’t report only “depression.” Report fatigue, concentration changes, cold intolerance, shortness of breath, pale skin, restless sleep, or heavy menstrual blood loss if those apply. Details change decisions.
A complete plan may involve a primary care clinician, a psychiatric nurse practitioner, therapy, medication, and lab assessment working together. For Pennsylvania residents who want remote access to medication management and whole-person depression care, this page on online depression treatment in Pennsylvania explains what telepsychiatry care can look like.
People who are still sorting through options may also find value in this overview of understanding depression treatment choices, especially if they’re trying to compare screening, evaluation, and treatment routes before scheduling care.
Frequently Asked Questions
Can someone just start taking iron on their own if they feel depressed and tired
Self-treating with iron is not a good first step. Depression, exhaustion, poor focus, and low motivation can come from iron deficiency, but they can also come from B12 deficiency, thyroid problems, sleep disorders, medication effects, blood loss, or depression itself. Iron can also be harmful when it is taken unnecessarily or in the wrong amount.
In practice, I advise patients to ask for testing before starting supplements. A CBC, ferritin, iron studies, B12, and folate usually give a much clearer picture of whether low iron is part of the problem.
If iron is low, how quickly does mood improve
It depends on the cause and the severity of the deficiency. Some people notice better stamina and less brain fog first. Mood often improves more gradually.
The timeline also changes if depression has more than one driver. If iron deficiency is present alongside major depressive disorder, trauma, chronic stress, poor sleep, or another medical issue, treatment needs to address each piece rather than waiting for one fix to solve everything.
Does treating anemia mean antidepressants are no longer needed
Sometimes yes. Often no.
If low iron or anemia is driving much of the fatigue, apathy, and poor concentration, correcting it can lead to a meaningful shift in mood. But many patients still benefit from therapy, antidepressant treatment, or both. Integrative psychiatry does not force a choice between medical and psychiatric care. It looks for the full set of contributors and treats them together.
Is over-the-counter oral iron always enough
Oral iron is a common starting point, but it is not always enough. Some patients do not absorb it well. Others stop because of constipation, nausea, or stomach pain. In those cases, the treatment plan may need to change, and the reason for the deficiency still needs attention.
That is one reason follow-up matters. If symptoms continue and labs are not improving, it is time to revisit the diagnosis, the dose, the treatment route, and possible sources of ongoing blood loss or poor absorption.
What if labs are only “borderline”
Borderline results can still matter, especially when the symptom pattern fits. A person can feel drained, foggy, irritable, and emotionally flat before anemia becomes severe on a standard CBC.
Clinical judgment is key. Lab interpretation should be tied to symptoms, medical history, menstrual history if relevant, diet, and any signs of gastrointestinal blood loss or absorption problems.
If depression, fatigue, and brain fog have not improved the way they should, a broader medical and psychiatric review may be the missing step. Integrative Psychiatry of America offers online psychiatric care in Pennsylvania with attention to lab screening, medication management, and treatment planning that addresses both mood symptoms and biological factors that may be contributing.

