Deadlines are slipping. Emails are half-finished. A simple household task turns into six unfinished steps. Many adults reach the point where they start asking whether this is stress, burnout, anxiety, or ADHD that was never fully recognized.
That question matters, but the next one matters even more. If ADHD is part of the picture, what kind of treatment will help day-to-day life feel more manageable?
ADHD medication can be a strong tool, but it works best when it’s handled as part of a partnership between patient and prescriber. Psychiatric nurse practitioners don't just match symptoms to a pill. Good care looks at attention, sleep, appetite, anxiety, medical history, work demands, routines, and whether a plan will be realistic to follow over time. That’s where medication management becomes more than prescribing. It becomes a practical, whole-person treatment process.
Table of Contents
- Is ADHD Medication the Right Path for You
- The Two Main Paths of ADHD Medication
- A Deep Dive into Stimulant Medications
- Exploring the Role of Non-Stimulant Medications
- Beyond the Prescription Integrative Complements
- Personalizing Your Treatment Dosing Monitoring and Adherence
- ADHD Medication Management via Telehealth in Pennsylvania
Is ADHD Medication the Right Path for You
The right starting point isn't, "Should a pill fix this?" The better question is, "What support plan matches the problems showing up in real life?" For one adult, the biggest issue is missed deadlines and mental clutter. For another, it's impulsive spending, emotional reactivity, or chronic difficulty finishing tasks even when they care a lot about the outcome.
A thoughtful evaluation looks at more than distractibility. It also asks whether symptoms have been persistent, whether anxiety or depression are overlapping, whether sleep is poor, and whether substance use, trauma, or medical conditions may be complicating the picture. Medication can help. It isn't the whole treatment plan.
For adults comparing next steps, this overview of ADHD treatment options for adults can help frame what usually comes before and after a prescription decision.
What makes medication a good fit
Medication tends to make sense when ADHD symptoms are interfering with work, relationships, parenting, school, or basic daily function. It may also be worth considering when someone has already tried planners, alarms, therapy, or self-help strategies and still feels like the brain won't reliably "hold the line" long enough to follow through.
A practical medication conversation usually includes:
- Target symptoms: What needs to improve first, focus, impulsivity, emotional regulation, task initiation, or consistency?
- Daily rhythm: Does the person need coverage mainly for work hours, evenings at home, or both?
- Medical context: Blood pressure, cardiac history, sleep, appetite, and other medications matter.
- Risk tolerance: Some people want fast symptom relief. Others care more about a steady, lower-burden option.
Clinical perspective: The best ADHD medication plan is the one a patient can tolerate, understand, and actually sustain.
For people who aren't sure whether their symptoms warrant formal treatment yet, it can help to speak to a medical expert and sort through the pattern before making assumptions. That kind of conversation can reduce stigma and prevent self-diagnosis from becoming the whole story.
What medication can and can't do
Medication may improve the brain's ability to filter distractions, sustain effort, pause before acting, and stay with a task long enough to finish it. What it doesn't do is automatically build routines, repair burnout, or teach organizational systems. That’s why good ADHD care usually combines medication with skills, structure, and lifestyle supports.
The Two Main Paths of ADHD Medication
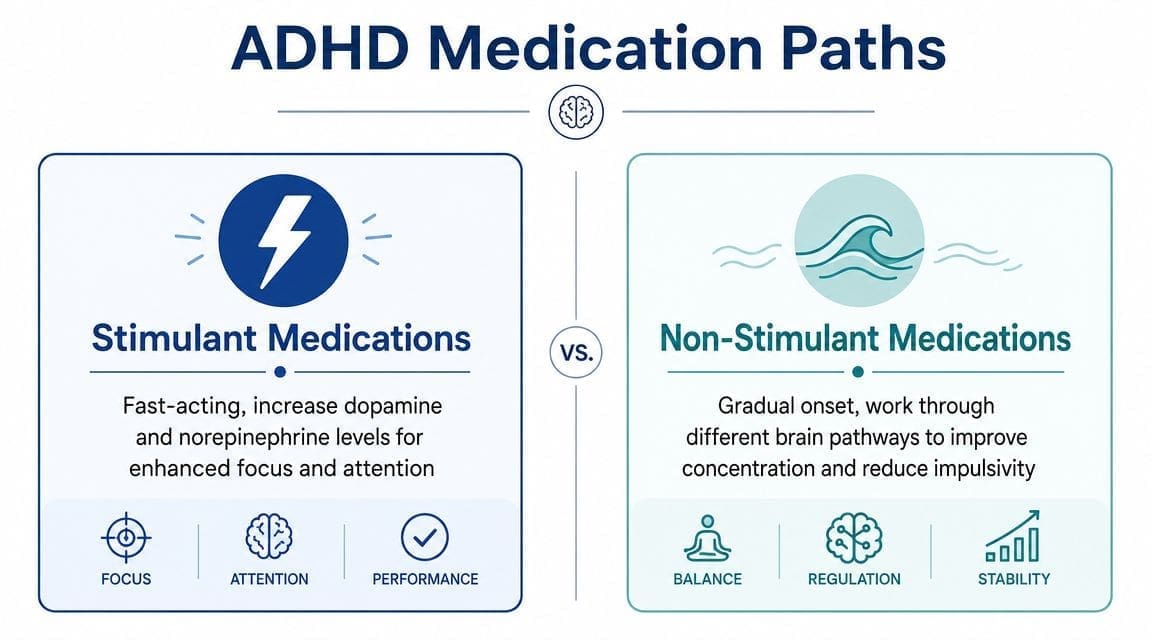
There are two main categories of ADHD medication. Stimulants are the older and more familiar path. Non-stimulants offer a different route and, for some patients, a better one.
Historically, stimulant treatment came first. The history of ADHD medication began in 1937 with stimulant use, and 2002 marked FDA approval of Strattera (atomoxetine), the first major non-stimulant option, as detailed in this history of ADHD pharmacotherapy. That timeline matters because it explains why many people still assume stimulants are the default and everything else is secondary.
How the two paths feel different
A simple way to think about it is this. Stimulants often act more like a light switch. Patients may notice effects relatively quickly. Non-stimulants are closer to a dimmer that gradually tunes the system over time.
That doesn't mean one is always stronger or better. It means they solve the same problem through different patterns of effect.
Some patients prefer a medication that feels clearly active and easier to notice. Others want something steadier, without controlled-substance logistics or abrupt wear-off periods. The right choice often depends on a patient's full clinical picture, not just symptom severity.
Some patients need speed. Others need steadiness. Matching the medication to the person usually works better than following habit or hype.
Stimulant vs. Non-Stimulant ADHD Medications at a Glance
| Feature | Stimulant Medications | Non-Stimulant Medications |
|---|---|---|
| Common examples | Methylphenidate products, amphetamine products | Atomoxetine, viloxazine, guanfacine |
| Onset pattern | Often faster acting | More gradual |
| Typical role | Commonly used first | Often used when side effects, access issues, anxiety, or misuse risk matter |
| Controlled substance status | Schedule II | Not Schedule II |
| Refill logistics | More regulated | Usually simpler |
| Best fit for some patients | Those needing more immediate symptom relief | Those wanting stable long-term management with fewer controlled-substance hurdles |
The most useful decision isn't stimulant versus non-stimulant in the abstract. It's whether the medication style fits the person's nervous system, health profile, and actual life.
A Deep Dive into Stimulant Medications
Stimulants are often the first medications discussed. They remain a core part of adult ADHD treatment because, for many patients, they improve attention, reduce impulsivity, and make task completion feel less effortful.
Methylphenidate and amphetamine options
The two main stimulant families are methylphenidate-based medications and amphetamine-based medications.
Methylphenidate works by blocking dopamine and norepinephrine transporters. It’s FDA-approved for ADHD in children age 6 and older and adults. According to this methylphenidate clinical review, adult doses average 20 to 30 mg/day, and dosing shouldn't exceed 60 mg/day because benefits plateau while risks rise.
That matters in real practice. More medication isn't automatically better medication.
Common methylphenidate products include Ritalin and longer-acting formulations such as Concerta. Amphetamine products include medications such as Adderall XR and lisdexamfetamine. Patients often describe the differences less in technical terms and more in lived terms. One may feel smoother, another may feel stronger, and another may wear off in a way that creates irritability or fatigue later in the day.
For readers comparing formulations and prescribing logistics, this guide on an Adderall prescription near me explains some of the practical issues patients often run into.
What monitoring actually looks like
Choosing a stimulant isn't the final step. Titration is where the work happens. A prescriber typically starts low, then adjusts based on symptom response, appetite, sleep, heart rate, blood pressure, and the patient's report of how the medication feels across the day.
Common trade-offs include:
- Appetite suppression: Some patients need meal planning because they forget to eat once the medication starts working.
- Sleep disruption: Timing matters. A dose taken too late can make bedtime harder.
- Physical activation: Jitteriness, increased heart rate, or feeling "too on" may mean the dose or formulation isn't right.
- Emotional rebound: Some people do well in the first half of the day, then crash when medication wears off.
A brief visual walkthrough can help make these differences easier to understand.
The goal isn't to force a stimulant to work. The goal is to see whether a stimulant works well enough, cleanly enough, and consistently enough to earn a place in the treatment plan.
Exploring the Role of Non-Stimulant Medications
Non-stimulants are often presented as the backup plan. That framing is too narrow. For some adults, a non-stimulant ADHD medication is the more practical first choice.
A key reason is that non-stimulants don't carry Schedule II restrictions. This discussion of non-stimulants being undervalued notes that they may have comparable efficacy in many cases while avoiding refill delays, regulatory burdens, and pharmacy supply problems that can interrupt care.
Who may benefit first
Non-stimulants deserve serious consideration when a patient has:
- Significant anxiety: A medication with a steadier onset may feel easier to tolerate.
- Concerns about misuse risk: Non-controlled options reduce that burden.
- Poor experiences on stimulants: Appetite loss, insomnia, or feeling overstimulated may push treatment in another direction.
- Telehealth access challenges: Simpler refill logistics can support consistency.
Examples include atomoxetine (Strattera), viloxazine (Qelbree), and guanfacine (Intuniv). They don't all work the same way, and they don't feel the same in the body. What they share is a more gradual pattern.
What patients should expect
The biggest mistake with non-stimulants is expecting a stimulant-style experience. These medications often don't produce a dramatic first-day shift. Improvement may show up more subtly. The patient may be less reactive, more organized, or less likely to abandon tasks midway through the week.
Important distinction: A medication doesn't have to feel intense to be effective. Some of the best ADHD treatment results look like steadier mornings, fewer arguments, and less chaos.
Non-stimulants can also fit naturally into longer-term, whole-person treatment. Patients who value consistency, fewer pharmacy disruptions, and lower administrative friction often find that these medications support adherence better than expected.
Beyond the Prescription Integrative Complements
A common pattern in ADHD treatment looks like this. The medication helps during part of the day, but the patient is still skipping meals, sleeping irregularly, losing track of tasks, and feeling frustrated by the gap between "better focus" and "better functioning." That gap matters, and it is where good medication management becomes a partnership instead of a refill process.
Medication works better with support around it
ADHD medication can reduce symptoms. It cannot organize a schedule, repair chronic sleep debt, or prevent the afternoon crash that follows too little food and too much caffeine. In practice, the patients who do best usually have both. A medication plan that fits their brain, and daily supports that fit their life.
The basics are not glamorous, but they change outcomes:
- Food timing: Regular meals can reduce irritability, headaches, and appetite-related crashes, especially with stimulants.
- Exercise structure: Planned movement often helps restlessness, stress tolerance, and sleep later that night.
- Mindfulness practice: This can strengthen pause, self-awareness, and emotional regulation, even when attention is still inconsistent.
- Behavioral supports: Calendars, reminders, visual cues, coaching, and simplified routines reduce the load on working memory.
Nutrition deserves special attention because blood sugar swings, low protein intake, and inconsistent eating can blur the picture. Patients may assume the medication is failing when the problem is under-fueling, rebound hunger, or poor sleep. This overview of how nutrition affects mental health explains that connection in more detail.
Where personalization adds value
Medication management should account for the whole clinical picture. Sleep patterns, anxiety, depression, trauma history, substance use, hormonal shifts, medical conditions, and drug interactions all affect how ADHD treatment feels day to day.
I often tell patients and families that our job is not just to ask, "Is the medication working?" The better question is, "What is helping, what is getting in the way, and what needs to change for this to be sustainable?" Sometimes the answer is a routine change. Sometimes it is therapy, coaching, school or workplace accommodations, or a closer look at sleep. Sometimes it is a medication adjustment.
Some practices also use genetic or lab-informed evaluation in selected cases when the response pattern is hard to explain or side effects appear early. That does not replace careful prescribing. It adds context.
One telepsychiatry option available to adults in Pennsylvania is Integrative Psychiatry of America, which combines medication management with nutrition education, mindfulness, exercise counseling, and related psychiatric support through virtual care.
Medication tends to work best when the treatment plan fits the patient's real life. The strongest ADHD care plans include prescribing, follow-up, and practical supports that the patient can keep using once the appointment ends.
Personalizing Your Treatment Dosing Monitoring and Adherence
A prescription only starts the process. The more important work is finding the dose and routine that a patient can maintain without feeling worse in other areas.
Why titration matters
Titration means adjusting the medication carefully instead of jumping to a fixed dose and hoping for the best. With stimulant treatment, this may involve small dose increases while watching focus, appetite, sleep, pulse, and blood pressure. With non-stimulants, it often means allowing enough time to judge a medication fairly before deciding it failed.
Patients should expect follow-up questions that are concrete, not vague:
- What got easier at work or home?
- What time of day does the medication help most?
- What side effects showed up, and when?
- Is the medication helping enough to justify staying on it?
This is also where tools like genetic testing for mental health may come up in selected cases, especially when the response pattern is uneven or medication tolerability has been difficult across several trials.
Why people stop medication even when it helps
One of the most overlooked parts of ADHD care is adherence. Fewer than half of adults with ADHD maintain consistent medication use, and early follow-up within the first 3 months improves adherence significantly, according to this discussion of adult ADHD medication nonadherence and solutions.
That finding matters because many people assume stopped medication means the treatment didn't work. Often, the underlying problem is different.
Barriers commonly include:
- Cost and coverage problems
- Refill friction
- Forgetting to request follow-up
- Side effects that were never adjusted
- Shame about needing help
- Unclear goals, so benefit becomes hard to measure
When a patient disappears after the first prescription, the answer usually isn't "they weren't motivated." The answer is often that the system made staying on treatment too hard.
The most effective monitoring plans reduce friction. They use early check-ins, clear symptom targets, simple refill processes, and honest discussion about what's getting in the way.
ADHD Medication Management via Telehealth in Pennsylvania
A common Pennsylvania telehealth visit starts this way: a patient logs in after months of missed deadlines, mounting frustration, and a growing sense that daily life is harder than it should be. The goal of that first appointment is not just to decide whether to prescribe. It is to understand the full picture, rule out look-alikes, and build a treatment plan that can hold up in real life.
Telehealth works well for ADHD care when it is organized and relationship-based. Medication management is rarely a one-visit decision. It usually involves an evaluation, review of records when available, screening for anxiety, depression, trauma, sleep problems, and substance use, plus a medical history that includes blood pressure concerns, heart history, and current medications.
The early steps often include:
- Scheduling and intake paperwork: insurance review or self-pay discussion, symptom forms, and consent
- Diagnostic assessment: childhood history, school or work impairment, and current patterns of inattention, impulsivity, or disorganization
- Safety and medical review: cardiovascular history, sleep, appetite, other psychiatric symptoms, and potential medication interactions
- Shared treatment planning: deciding whether medication fits, which class makes sense, and what non-medication supports should be added
Patients who want a clearer picture of how virtual care is structured can review online psychiatry in Pennsylvania for ADHD care.
What makes telehealth useful is not convenience alone. It gives patients and prescribers more chances to adjust treatment before small problems turn into treatment drop-off. If a stimulant helps focus but disrupts sleep, or a non-stimulant improves consistency but causes fatigue, follow-up can happen quickly enough to respond. That kind of back-and-forth is the core of good ADHD medication management.
Privacy also matters. Secure platforms, clear documentation practices, and thoughtful use of digital tools all affect patient trust. For a plain-language overview of online privacy concerns, this guide on understanding healthcare AI risks is a useful starting point.
For adults in Pennsylvania, good telehealth ADHD care should feel clear, responsive, and collaborative. The best visits leave the patient knowing what medication is for, what side effects to watch for, what happens with refills, and when to follow up. That is how treatment becomes more than a prescription.
Adults in Pennsylvania who want a structured, whole-person approach to adhd medication, evaluation, and follow-up can learn more through Integrative Psychiatry of America. The practice provides online psychiatric care with medication management, lifestyle support, and secure telehealth visits designed to make treatment easier to start and easier to continue.

