
A lot of searches for Tricare for depression Philadelphia Pennsylvania start the same way. Someone is awake late, scrolling on a phone, trying to answer a few urgent questions without having to explain everything out loud yet. Is therapy covered? Are antidepressants covered? Is virtual care allowed? What happens if symptoms are getting worse and treatment needs to start soon?
That moment is common in Philadelphia, Pittsburgh, Allentown, Harrisburg, Erie, Scranton, Lancaster, Reading, and across the state. Depression already makes decision-making harder. Insurance questions add another layer of friction. Many people aren't looking for a lecture on brain chemistry. They want a practical path that helps them feel better and avoids insurance surprises.
For most, outpatient care usually begins with TRICARE outpatient mental health treatment, which serves as the primary entry point for care, with standard outpatient services including weekly or biweekly individual or group therapy and psychiatric evaluations, where approximately 36.2% of all individuals seeking mental health care initiate treatment at this level according to Mission Connection Healthcare's overview of TRICARE mental health coverage. For many adults with depression, that means starting with an evaluation, discussing therapy, and deciding whether medication makes sense.
Patients who are exploring depression treatment options in Pennsylvania often need two things at once. They need clear clinical guidance, and they need realistic answers about access. Both matter.
A medication discussion should feel grounded and collaborative. Some people are worried about side effects. Others are afraid medication will change their personality. Some have tried one medication before and stopped because the first weeks were rough. Those concerns are valid, and they should be part of the decision.
Table of Contents
- Your Search for Depression Treatment in Pennsylvania
- Understanding Your TRICARE Mental Health Benefits
- Antidepressants 101 SSRIs and TCAs Explained
- A Detailed Patient-Focused Comparison of SSRIs and TCAs
- How Your Provider Chooses the Right Medication for You
- Practical Guidance for Medication Management and Safety
- Begin Your Path to Treatment With Virtual Care
Your Search for Depression Treatment in Pennsylvania
A typical search begins subtly. An adult in Center City Philadelphia might be trying to keep up at work while feeling flat, exhausted, irritable, or numb. Another person in Pittsburgh may already know they're depressed but keeps delaying care because insurance rules feel confusing. Someone in Allentown may wonder whether telehealth is “real treatment” or only a temporary option.
Depression often narrows a person's world before treatment begins. Tasks feel heavier. Sleep may shift in either direction. Concentration gets worse. Simple choices like whether to book an appointment or refill a medication can feel unreasonably hard.
What people usually want to know first
Most patients don't begin by asking for a specific drug. They start with practical questions.
- Is this serious enough for treatment Some people minimize symptoms for months before reaching out.
- Will TRICARE cover care Insurance uncertainty keeps many people stuck.
- Can this be handled virtually Adults in Philadelphia and across Pennsylvania often want confidential treatment from home.
- Will medication help, or make things worse first That fear is common and worth discussing directly.
A useful first step is understanding that outpatient care is the normal place to begin for many people. That often includes an evaluation, follow-up visits, therapy referrals or coordination, and medication management when appropriate.
Many patients don't need a dramatic crisis to justify care. Persistent sadness, loss of interest, low motivation, sleep change, guilt, hopelessness, or trouble functioning are enough reasons to get evaluated.
The search for Tricare for depression Philadelphia Pennsylvania is rarely only about insurance. It's usually about trying to find a path that feels manageable. For some, that means starting therapy. For others, it means discussing medication because symptoms are interfering with work, parenting, school, or relationships.
Why the first appointment matters
The first visit should reduce confusion, not add to it. A strong depression evaluation usually clarifies:
| Question | Why it matters |
|---|---|
| What symptoms are present | It helps distinguish depression from burnout, grief, anxiety, trauma, or bipolar-spectrum concerns |
| How severe symptoms are | This guides urgency and level of care |
| Whether medication fits | Not every patient needs the same approach |
| What TRICARE may cover | Treatment planning works better when benefits are clear |
| Whether virtual follow-up is realistic | For many adults in Pennsylvania, it is |
That kind of clarity matters whether someone lives in Philadelphia, Harrisburg, Erie, Scranton, or Reading. Depression treatment works best when access is simple enough that people can stay in care.
Understanding Your TRICARE Mental Health Benefits
TRICARE does cover a meaningful range of depression treatment. That's the part many patients need to hear clearly. The starting point for most adults is outpatient care, and TRICARE recognizes that.
TRICARE covers office-based outpatient psychotherapy for depression when medically or psychologically necessary, including individual crisis sessions and regular individual sessions. TRICARE explicitly covers psychotropic drugs for depression when prescribed by an authorized provider as part of a treatment plan, according to the TRICARE covered mental health therapeutic services page.
What that means in practice
For a patient in Pennsylvania, that usually means several core services may be part of care:
- Therapy visits Individual, family, conjoint, and group formats may be covered when medically necessary.
- Medication treatment Antidepressants and other psychiatric medications can be covered when they're part of an authorized treatment plan.
- Testing and assessment Psychological testing and assessment may be covered when needed for diagnosis and treatment planning.
- Additional interventions Certain higher-level treatments may also be covered when criteria are met.
A lot of confusion comes from not knowing whether an evaluation and medication follow-up count as legitimate mental health treatment under the plan. They do, when delivered within TRICARE rules and medical necessity standards.
Telehealth matters in Pennsylvania
Telepsychiatry is especially relevant in a state as geographically broad as Pennsylvania. A patient in Philadelphia may choose virtual care for convenience and privacy. A patient in Erie or Scranton may choose it because local scheduling is limited. Someone in Lancaster or Reading may want shorter travel time and easier follow-up.
That's one reason many people specifically search for Tricare for depression Philadelphia Pennsylvania instead of only “depression treatment.” They're not just looking for a diagnosis. They're trying to figure out whether real treatment can happen in a format that fits daily life.
Coverage rule: It's smart to verify the provider network status and whether a referral is needed under the specific TRICARE plan before the first appointment.
Patients looking for plan-specific guidance can review TRICARE military insurance information for mental health care in Pennsylvania to understand the practical next steps before booking.
A few insurance questions worth asking upfront
Before starting care, it helps to confirm:
- Plan type Prime, Select, and Reserve Select can differ in how care is accessed.
- Network status In-network and out-of-network logistics aren't the same.
- Referral requirements Some services may be easier to access than patients expect, but it's still worth checking.
- Pharmacy details Medication coverage often depends on formulary and prescribing rules.
Insurance shouldn't be the reason someone stays untreated. But it does help to start with accurate expectations.
Antidepressants 101 SSRIs and TCAs Explained
Medication names can sound intimidating before a patient even gets to the question of whether one is a good fit. Two categories that often come up in depression treatment are SSRIs and TCAs. They both treat depression, but they're not interchangeable in how they work, how they feel, or how providers usually use them.
TRICARE covers mental health treatment for conditions such as depression and anxiety in both inpatient and outpatient settings, with coverage depending on the specific plan and applicable limitations, as summarized by Recovery.com's Philadelphia TRICARE overview. For medication discussions, the more useful question is often which class makes the most sense for the individual patient.
What SSRIs are
SSRIs stands for selective serotonin reuptake inhibitors. In plain language, they increase the availability of serotonin in the brain. Serotonin is one of the chemical messengers involved in mood, anxiety, sleep, appetite, and emotional regulation.
These medications are often discussed early because they're commonly used for:
- Depression
- Anxiety disorders
- Obsessive compulsive symptoms
- Trauma-related symptoms in some patients
Patients who want a simple explanation of serotonin can review this patient-friendly overview of 5-HT and serotonin, since “5-HT” is another name that sometimes shows up in medication conversations.
What TCAs are
TCAs means tricyclic antidepressants. They're an older class of antidepressants that affect more than one neurotransmitter, including serotonin and norepinephrine. Because they work more broadly, they can be effective, but they also tend to come with a more complicated side effect and safety profile.
TCAs are still used. They haven't disappeared from practice. They're typically less likely to be the first medication offered for many adults with uncomplicated depression.
SSRIs are often easier for patients to start and tolerate. TCAs can still be useful, but they usually require more caution and closer monitoring.
Why the difference matters
For patients, this isn't a chemistry lesson for its own sake. It matters because medication choices affect day-to-day life. An antidepressant isn't only about whether mood improves. It's also about whether the patient can sleep, work, focus, tolerate the side effects, and safely continue treatment long enough to know if it helps.
A patient with depression and panic symptoms may hear more about SSRIs. A patient with a more complex history, certain pain conditions, or prior medication failures may hear TCAs mentioned. The class itself doesn't decide the answer. The patient's symptom pattern, health history, and tolerability do.
A Detailed Patient-Focused Comparison of SSRIs and TCAs
This side-by-side view helps make the trade-offs clearer. The goal isn't to label one class “good” and the other “bad.” The central question is which one fits the patient sitting in front of the clinician.
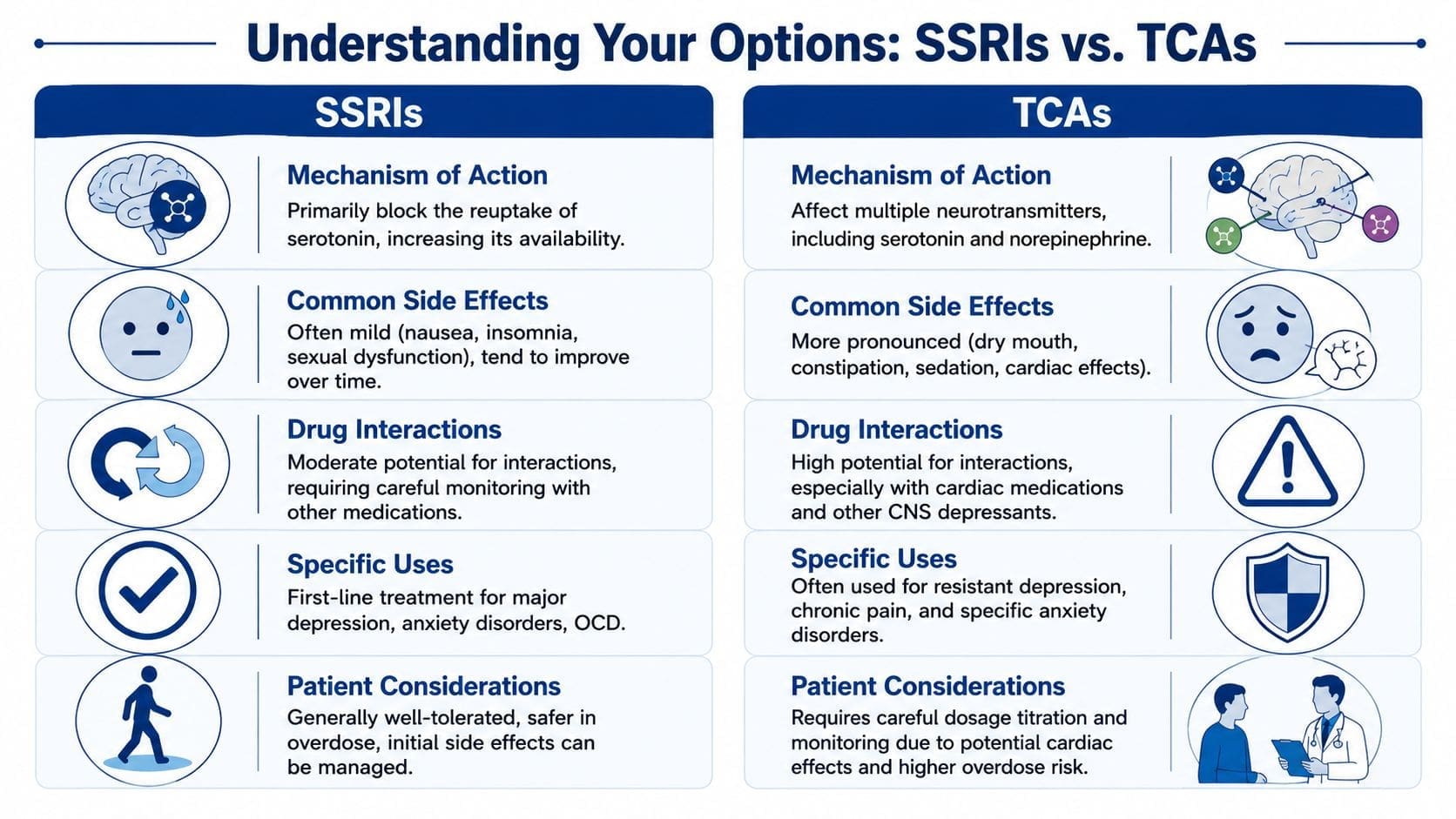
| Feature | SSRIs | TCAs |
|---|---|---|
| Typical role | Often considered first-line for many patients with depression | Often considered when specific clinical reasons support their use |
| Neurotransmitters affected | Primarily serotonin | Multiple neurotransmitters, including serotonin and norepinephrine |
| Common tolerability pattern | Often easier to start, though early side effects can still be frustrating | Often harder to tolerate because side effects can feel more noticeable |
| Safety considerations | Generally viewed as safer in overdose than TCAs | Requires more caution because overdose risk is a bigger concern |
| Monitoring burden | Usually simpler | Often needs closer attention to interactions and side effects |
Side effects patients actually notice
Patients don't experience medications as textbook categories. They experience them as dry mouth during a meeting, nausea during breakfast, feeling sedated while trying to parent, or changes in sexual function that affect a relationship.
SSRIs often bring side effects such as:
- Nausea or stomach upset
- Headache
- Restlessness or insomnia
- Sexual side effects
- Sweating or feeling activated
These effects may improve with time, dose adjustment, or careful medication selection within the class.
TCAs more often raise concerns like:
- Dry mouth
- Constipation
- Sedation
- Dizziness
- Blurred vision
- Cardiac concerns in some patients
That doesn't mean every patient on a TCA feels worse. It means the burden of side effects is often more noticeable, especially early or at higher doses.
Depression with anxiety, OCD, or PTSD symptoms
SSRIs are commonly used when depression overlaps with anxiety or obsessive thinking. That matters because many patients don't have “pure” depression. They may have rumination, panic, trauma-related avoidance, or repetitive intrusive thoughts.
TCAs can still be useful in selected situations, but they're less often the first discussion when anxiety sensitivity is already high. If a patient is worried about feeling physically uncomfortable from medication, the side effect profile matters a lot.
A medication can be effective on paper and still be the wrong practical choice if the patient can't tolerate it long enough to benefit.
Safety and interaction trade-offs
The distinction holds greater weight than mere preference. TCAs usually require more caution with other medications and with certain medical conditions. Cardiac issues are an especially important consideration. That doesn't automatically rule them out, but it changes how prescribing is approached.
SSRIs aren't interaction-free. They can still affect other medications and need proper review. But in general practice, many providers consider them more straightforward to use safely for a broad range of adults.
When a TCA may still make sense
A TCA may come up when:
- Past SSRIs haven't worked well enough
- Side effects from several newer medications were not manageable
- A patient has symptom patterns or co-occurring issues that make a TCA worth considering
- There's a strong past personal or family response history
This is why blanket advice doesn't help much. The better question is not “Which one is stronger?” It's “Which one makes the most sense for this patient's symptoms, medical history, and daily life?”
How Your Provider Chooses the Right Medication for You

The best antidepressant is the one that fits the whole person, not just the diagnosis. Two patients can both meet criteria for depression and still need very different treatment plans. One may be slowed down, sleeping too much, and struggling to get out of bed. Another may be wired, panicky, and unable to fall asleep.
The clinical factors that shape the choice
A provider usually weighs several issues at once.
- Symptom pattern Depression with insomnia may lead to a different discussion than depression with fatigue.
- Co-occurring conditions Anxiety, OCD, PTSD symptoms, ADHD, chronic pain, and substance use all affect the medication decision.
- Medical history Cardiac conditions, seizure history, pregnancy considerations, and other medical issues matter.
- Current medications Interaction risk changes what is safe.
- Past response history If a medication helped before, that's useful information.
- Family response history Relatives sometimes respond similarly to certain medications.
- Patient preference Concerns about sedation, weight change, sexual side effects, or activation should shape the plan.
A thoughtful medication discussion also considers lifestyle. A night-shift worker in Philadelphia may not tolerate a highly sedating medication well. A college student in Pittsburgh may be especially concerned about concentration. A parent in Harrisburg may need a medication schedule that's simple enough to follow consistently.
When additional tools help
Sometimes the usual decision points are enough. Sometimes they aren't. In more complex cases, providers may consider lab review, broader medical screening, or pharmacogenomic support to help organize the next step. These tools don't replace clinical judgment, but they can add context.
Patients who are curious about this topic can learn more about genetic testing for psychiatric medications as part of a broader medication-planning discussion.
Clinical reality: A medication plan works better when it matches the patient's routine, health conditions, and side effect tolerance. A theoretically perfect medication isn't useful if the patient can't stay on it.
If first-line treatment doesn't work
Some patients improve with the first medication. Others need adjustments, a switch, augmentation, psychotherapy, or a different level of intervention. That's not treatment failure in a personal sense. It's part of psychiatric care.
For treatment-resistant depression, TRICARE covers Transcranial Magnetic Stimulation (TMS) specifically for treatment-resistant depression, requiring beneficiaries to be at least 15 years old and have failed to respond to two adequate trials of antidepressants across different categories plus a psychotherapy trial, as outlined in the TriWest TRICARE behavioral health coverage and requirements document.
That matters because it shows the treatment pathway doesn't stop at “try one SSRI and hope.” There are additional options when standard care hasn't been enough.
Practical Guidance for Medication Management and Safety
Starting medication is only the beginning. The early phase of treatment is where many patients need the most support, because improvement often isn't immediate and side effects may show up before benefits do.
What the first few weeks can feel like
Some patients feel almost nothing at first. Others notice stomach upset, mild activation, sleep change, or fatigue before mood improves. That doesn't always mean the medication is wrong. It does mean follow-up matters.
A practical approach usually includes:
- Tracking symptoms Mood, sleep, appetite, anxiety, focus, and side effects are easier to review when written down.
- Watching function Getting out of bed, completing work, and staying engaged with other people often improve before a patient says they “feel good.”
- Staying in contact Medication changes are safer when they happen through scheduled follow-up instead of abrupt self-adjustment.
Using a structured tool can make telehealth visits much more productive. A simple mood and side-effect record such as a Feeling Journal for symptom tracking helps patients notice patterns they may otherwise forget by appointment day.
Don't stop suddenly without guidance
Many antidepressants should not be stopped abruptly. Even when a medication isn't helping, it often needs a taper rather than a sudden stop. The right discontinuation plan depends on the medication, the dose, how long the patient has taken it, and what's being started next.
This is especially important when patients are discouraged. It's understandable to want to quit a medication after a rough week. But making changes without guidance can create unnecessary withdrawal symptoms, return of depression, or confusion about what the body is reacting to.
If a medication feels wrong, the answer usually isn't silence or abrupt discontinuation. The safer move is a prompt follow-up visit and a clear adjustment plan.
A common TRICARE misunderstanding in Pennsylvania
One insurance misunderstanding deserves direct correction because it can affect safety planning. A critical underserved angle is the widespread misconception that TRICARE covers residential mental health treatment for adults in Pennsylvania; data confirms that residential care is only a covered benefit for beneficiaries under 21, while adult residential treatment is explicitly excluded except for substance use disorder, according to Rock View Recovery's explanation of TRICARE mental health coverage.
This matters for adults in Philadelphia and throughout Pennsylvania who assume residential depression treatment is available under TRICARE when symptoms escalate. For adult non-substance mental health conditions, that assumption can delay realistic planning. Patients and families may need to consider other covered levels of care, such as outpatient, intensive outpatient, partial hospitalization, emergency evaluation, or inpatient services when clinically appropriate.
Medication management works best when expectations are realistic
A strong treatment plan usually includes:
- A target list What exactly needs to improve first.
- A follow-up schedule So dose changes and side effects are reviewed, not guessed at.
- A safety plan Especially if hopelessness, suicidal thoughts, or rapid worsening are present.
- A backup path Therapy adjustment, medication switch, or advanced treatment if the first plan doesn't work.
Depression treatment is often a process of adjustment, not a single perfect prescription.
Begin Your Path to Treatment With Virtual Care
For adults searching for Tricare for depression Philadelphia Pennsylvania, virtual care can remove some of the biggest barriers to getting started. It makes evaluations, medication follow-up, and ongoing treatment easier to fit into real life across Philadelphia, Pittsburgh, Allentown, Harrisburg, Erie, Scranton, Lancaster, Reading, and other Pennsylvania communities.
Telehealth also helps when the hardest part is beginning. A patient can start with a confidential evaluation from home, review medication options carefully, and build a treatment plan that matches both symptoms and insurance realities. For people who also want a general overview of how online prescribing works, this guide to Blue Haven RX prescriptions can be a useful supplemental resource alongside provider-specific instructions.
Patients who are ready to explore online care for depression in Philadelphia often benefit most from one simple next step. Book the evaluation, verify benefits, and bring a clear list of symptoms, past medications, and questions. That's often enough to turn a stalled search into an actual treatment plan.
If depression has been affecting daily life, Integrative Psychiatry of America offers virtual psychiatric evaluations, medication management, and evidence-informed mental health treatment across Pennsylvania. Patients can learn more about treatment options, verify insurance coverage, schedule an appointment, or use free tools such as the Adult ADHD Assessment, Anxiety Symptom Checker, Daily Agenda Planner, Feeling Journal, Exercise Routine Generator, and 5-4-3-2-1 Grounding Tool to take the next step.

