Some people search how does Wellbutrin work after months of feeling unlike themselves. The sadness may be there, but often the bigger problem is heavier than sadness. Getting out of bed feels mechanical, work takes twice the effort, exercise disappears, meals get irregular, and even enjoyable things feel flat.
That pattern matters because not every antidepressant works the same way. Some people have already tried a serotonin-focused medication and felt emotionally less sharp, more tired, or frustrated by sexual side effects or weight changes. Others haven't tried medication yet, but want to understand why one option might fit better than another.
For adults in Pennsylvania using telepsychiatry, Wellbutrin is often worth understanding in plain language. It has a different mechanism, a different feel, and a different set of trade-offs than many common antidepressants. It can be especially relevant when depression shows up as low energy, reduced motivation, poor focus, or a hard time re-engaging with therapy, movement, and routine. The role of nutrition also matters in recovery, which is why many patients find it helpful to also learn how nutrition affects mental health.
Table of Contents
- A Different Approach to Feeling Better
- How Wellbutrin Uniquely Works in Your Brain
- Clinical Uses for Wellbutrin Treatment
- Your Treatment Timeline What to Expect Week by Week
- Navigating Dosing Side Effects and Safety
- Wellbutrin in Your Integrative Telepsychiatry Plan
- Frequently Asked Questions About Wellbutrin
- Partnering For Your Mental Wellness Journey
A Different Approach to Feeling Better
From the outside, depression can look like simple fatigue or disinterest. I see this often with patients across Pennsylvania who are still getting through work, answering family texts, and meeting obligations, but inside they feel flat, slowed down, and disconnected from any sense of reward. In that situation, the primary question usually is not just, “What treats depression?” It is, “What might help me get my drive back?”
Wellbutrin, the brand name for bupropion, comes up in that conversation because it tends to feel different from many antidepressants patients have heard about before. In practice, it is often considered when depression shows up as low energy, poor initiation, reduced focus, or a sense that everything takes too much effort.
That difference matters in real life. Medication choice is partly about symptom relief, but it is also about trade-offs. Sleep can improve or worsen. Appetite may shift. Sexual side effects matter. Anxiety sensitivity matters. The best fit is the medication whose benefits line up with the patient’s symptom pattern and whose downsides are manageable in daily life.
As a board-certified psychiatric nurse practitioner at Integrative Psychiatry of America, I explain Wellbutrin to patients as a medication that may help remove some of the drag that keeps recovery stuck. If a person starts to feel enough activation to take a walk, prepare actual meals, participate in therapy, or follow through on routines, the medication is supporting more than mood. It is helping create the conditions that let an integrative treatment plan work.
That is where the patient experience becomes important. Early gains with Wellbutrin are often less about suddenly feeling happy and more about noticing a little more mental traction. A task feels slightly easier to start. Getting out of bed takes less negotiation. That shift can make it more realistic to work on the other pieces of care, including sleep habits, movement, therapy, and how nutrition affects mental health.
For many patients, that is the value of this medication. It can support the energy and motivation needed to participate in recovery, not just observe it from the sidelines.
How Wellbutrin Uniquely Works in Your Brain
The messenger system behind motivation and energy
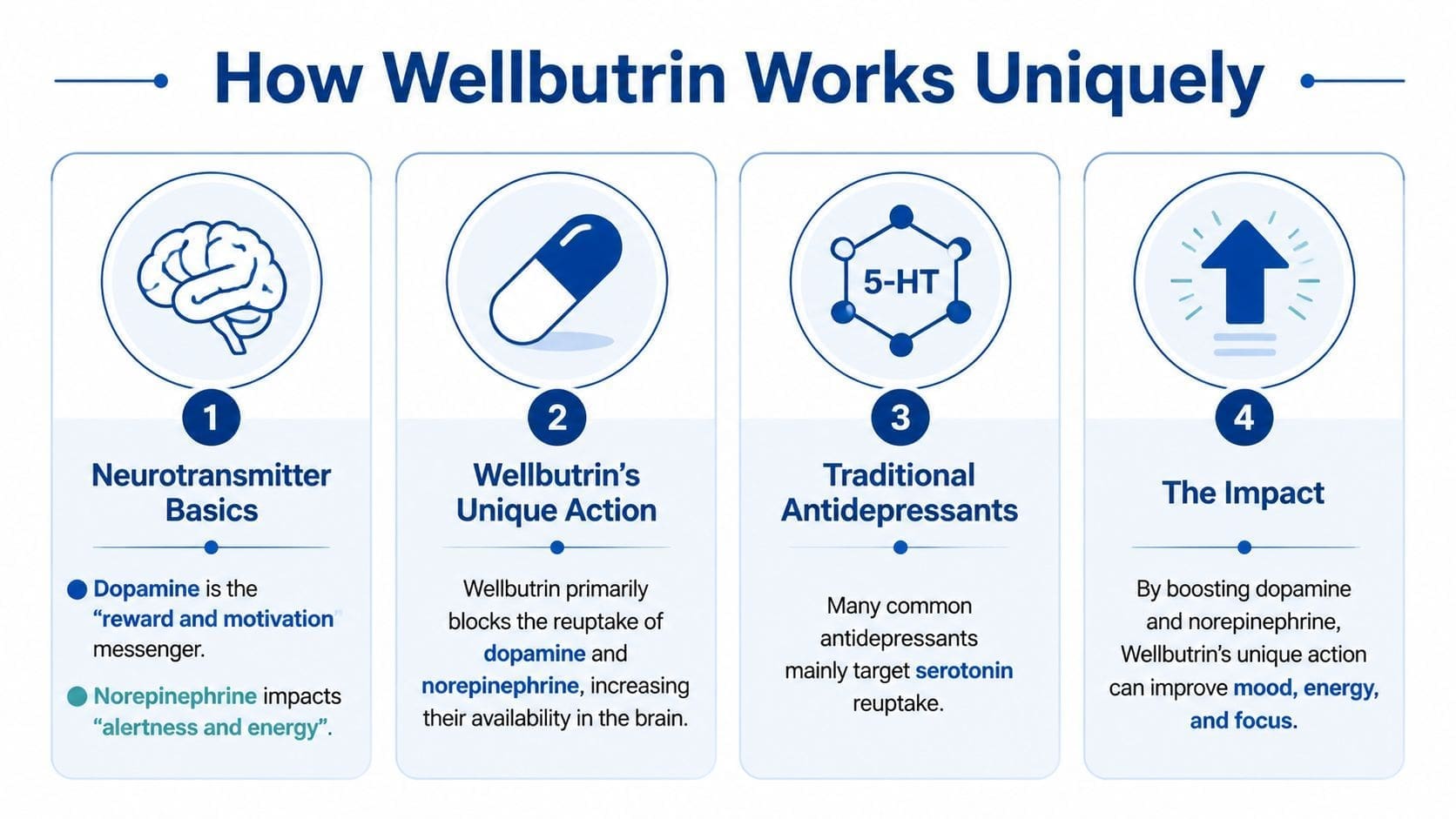
To understand how does Wellbutrin work, start with two brain chemicals that shape day-to-day functioning: dopamine and norepinephrine. In practice, these systems affect drive, focus, mental stamina, and the ability to get started on something that feels effortful.
Dopamine is tied to reward, interest, and follow-through. Norepinephrine is tied to alertness, attention, and readiness. When depression disrupts these pathways, patients in Pennsylvania often describe the result in very concrete terms. They are not only sad. They feel slowed down, foggy, unmotivated, and unable to shift from intention to action.
What NDRI really means
Bupropion is classified as an NDRI, short for norepinephrine-dopamine reuptake inhibitor. It slows the reabsorption of dopamine and norepinephrine after those chemicals are released between nerve cells. That gives these signals more time to do their job.
The StatPearls review of bupropion in the NCBI Bookshelf describes this mechanism as selective inhibition of norepinephrine and dopamine reuptake. Clinically, that helps explain why Wellbutrin often feels different from medications that work mainly through serotonin. It tends to match a symptom pattern that includes low drive, reduced pleasure, poor concentration, and mental inertia.
I often explain this to patients as a treatment that may improve traction. The goal is not artificial stimulation. The goal is to reduce the internal drag that makes basic tasks feel disproportionately hard. If that happens, a person may be more able to exercise consistently, eat regular meals, show up fully in therapy, and follow through with routines that support recovery.
For patients comparing options, it also helps to understand what 5-HT means in brain chemistry, because 5-HT is another name for serotonin.
Why it feels different from serotonin-first medications
Many antidepressants are SSRIs, which primarily affect serotonin. Wellbutrin does not target serotonin in the same way, and that difference often shows up in the patient experience.
Some people notice early changes as improved alertness, a little more willingness to start tasks, or less of that heavy, stalled feeling. Mood improvement usually takes longer than those first functional shifts. That timeline matters in integrative care, because even a modest increase in energy can make it easier to participate in therapy, movement, sleep work, and nutrition changes instead of waiting passively for medication to do everything.
There are trade-offs. A medication that feels activating for one person may feel too stimulating for another, especially if anxiety, insomnia, or jitteriness are already part of the picture. That is why prescribing Wellbutrin is not just about knowing its mechanism. It is about matching that mechanism to the person sitting in front of you.
A few practical points summarize why its mechanism stands out:
- Activation: Wellbutrin is often more energizing than sedating.
- Motivation: Its dopamine and norepinephrine effects can make it a reasonable option when depression includes apathy, low interest, or difficulty initiating tasks.
- Sexual side effects: It is often considered when patients want to avoid the sexual side effects commonly associated with serotonin-focused antidepressants.
- Attention and focus: The same mechanism is one reason bupropion comes up in conversations about ADHD symptoms.
Patients rarely describe this in neurochemical terms. They usually say, “I know what I need to do, but I cannot get myself to start.” That is often the symptom clue that makes Wellbutrin worth considering.
Clinical Uses for Wellbutrin Treatment
A patient in Pennsylvania might tell me, “I’m depressed, I can’t focus, and I want to quit smoking. Do I need three different medications?” Sometimes the answer is yes. Sometimes Wellbutrin is worth considering because one medication can address more than one problem at once.
That overlap is the practical reason bupropion comes up so often in psychiatric care. Its clinical uses are tied to the same activating profile, but the goal is never to force one medication to fit every situation. The goal is to match the medication to the symptoms, the person, and the full treatment plan.
Major depressive disorder
Wellbutrin is FDA-approved for major depressive disorder. In practice, I consider it most often when depression looks slowed down rather than agitated. Patients may describe low drive, mental fog, sleeping more than usual, less interest in daily life, or trouble getting started on simple tasks.
That symptom pattern matters.
A person who feels sad and tearful all day may need a different approach than a person who says, “I feel flat, stuck, and I cannot get moving.” Wellbutrin is often more appealing in the second situation, especially if preserving sexual function or avoiding daytime sedation is also a priority.
It also fits well with integrative treatment. If a medication helps a patient get out of bed, take a walk, cook a decent meal, or show up more fully in therapy, those gains can compound in a healthy way. Medication is not the whole plan. It can create enough momentum for the rest of the plan to work better.

Smoking cessation
Bupropion is also FDA-approved for smoking cessation under the brand name Zyban. The FDA prescribing information for Zyban describes its use as part of a quit-smoking plan.
Clinically, this makes sense. Nicotine affects reward circuits in the brain, and bupropion can reduce some of the reinforcement that keeps smoking going. Patients often ask whether it makes cigarettes taste bad or removes cravings completely. Usually, it does neither. What it may do is lower the intensity of the urge and make the quit attempt more manageable.
That distinction is important because smoking treatment still works best with structure. A quit date, behavioral strategies, support, and a clear plan for high-risk moments all matter. In telepsychiatry, we often pair medication with coaching around routines, stress triggers, sleep, meals, and movement, because nicotine relapse is rarely just about nicotine.
Adult ADHD off-label use
Bupropion is not FDA-approved for ADHD, but it is used off-label in some adults. The Cochrane review on bupropion for attention deficit hyperactivity disorder in adults found low-quality evidence that it may reduce ADHD symptoms more than placebo.
I discuss it as a second-line or situation-specific option, not a replacement for stimulant treatment across the board. Stimulants are usually more effective for core ADHD symptoms. Bupropion enters the conversation when someone also has depression, wants to avoid a controlled substance, has not tolerated stimulants well, or needs a plan that accounts for several goals at once.
That middle-ground role is one reason it comes up in more nuanced treatment decisions, including bupropion in ADHD medication decisions during pregnancy.
A practical summary:
- For depression: It may fit patients with low energy, low motivation, and reduced pleasure.
- For smoking cessation: It can support quitting by reducing the reward pull of nicotine and helping with withdrawal-related symptoms.
- For adult ADHD: It may help some adults who need a non-stimulant option, especially when depression is also part of the picture.
In my practice, Wellbutrin is most useful when the treatment target is broader than mood alone. If the plan is to improve energy, rebuild routine, increase follow-through, and make therapy, exercise, and nutrition easier to sustain, its mechanism can support that work in a very practical way.
Your Treatment Timeline What to Expect Week by Week
Patients often feel discouraged when they don't feel emotionally transformed after a few days. With Wellbutrin, that expectation usually causes unnecessary frustration because the timeline is often staggered.

Weeks 1 and 2
Early changes are often physical or behavioral before they are emotional. A person may notice it’s easier to get moving in the morning, the body feels a little less slowed down, appetite feels more regulated, or sleep patterns begin shifting.
That sequence is supported by Medical News Today’s discussion of Wellbutrin’s timeline, which notes that sleep, energy, and appetite often improve within 1 to 2 weeks, while mood and motivation changes usually take longer. Patients sometimes find this confusing. They may say, “I think something is changing, but I don't feel happier yet.”
That doesn't automatically mean the medication is failing. It may mean it is working in the expected order.
What helps most early on: Track concrete changes, not just mood. Getting out of bed faster, walking more consistently, finishing simple tasks, or eating on a steadier schedule all count.
Weeks 4 through 6
By this stage, the changes often become more recognizably antidepressant in the way patients expect. Interest may begin to return. Tasks may feel less impossible. There may be more emotional range, more initiative, and less time spent mentally pushing against basic responsibilities.
A short explanation can make this less abstract. Early energy changes can happen before deeper emotional patterns shift because activating neurotransmitter systems doesn't instantly rebuild habits, outlook, and coping patterns. The brain may become more ready for change before the person fully feels that change as improved mood.
This is also a useful point to reassess therapy goals, activity levels, and routine. More energy without structure doesn't automatically create recovery. More energy directed into treatment usually does.
A helpful visual summary appears below.
Why that sequence matters
When a patient understands the timeline, adherence usually improves. The early window is not just a waiting period. It's a chance to use any increase in activation to build momentum.
That might include:
- Movement: restarting walks, light exercise, or a gym routine
- Therapy work: showing up with enough focus to do meaningful cognitive or emotional work
- Nutrition: planning meals instead of grazing or skipping
- Daily structure: setting wake times, work blocks, and simple essential routines
The practical message is straightforward. If the body starts moving before the mood fully lifts, that's often the opening. It's the time to reinforce recovery habits instead of assuming the medication should do every part alone.
Navigating Dosing Side Effects and Safety
A common Pennsylvania telepsychiatry scenario goes like this. A patient starts Wellbutrin, notices a little more energy, then wonders whether dry mouth, trouble falling asleep, or feeling keyed up means the medication is wrong for them. In many cases, those early effects are manageable. The safer approach is to look at dose, formulation, timing, and personal risk factors before making a decision.
Wellbutrin can be a very good fit, but it is not a casual medication. As a board-certified psychiatric nurse practitioner, I pay close attention to how a patient sleeps, how much alcohol they use, whether they have an eating disorder history, whether anxiety is already running high, and what time of day they tend to feel most activated. Those details shape tolerability.
The main formulations
Bupropion comes in immediate-release, sustained-release, and extended-release forms. The release pattern affects how quickly the medication peaks and how smooth it feels across the day. Immediate-release tends to hit faster. Extended-release is usually steadier and often easier to fit into a morning routine. Sustained-release sits somewhere in the middle.
That difference matters in real life. A patient who is sensitive to stimulation may do better with a slower, steadier version. A patient who wants a simpler schedule may prefer once-daily dosing. The medication name stays the same, but the day-to-day experience can feel different depending on the formulation and when it is taken.
Patients who want a more individualized approach sometimes ask whether biology can help guide medication choices. Our overview of genetic testing for depression medication decisions explains where that tool may help and where standard clinical judgment still matters more.
Common side effects and what helps
Wellbutrin is often chosen because it has a different side effect profile than many serotonin-based antidepressants. In practice, that can mean fewer sexual side effects and less concern about weight gain for some patients. It can also mean more activation early on, which is useful for low motivation but less comfortable for someone who already feels tense, restless, or short on sleep.
The side effects I discuss most often are:
- Insomnia or lighter sleep: morning dosing often helps
- Dry mouth: water, sugar-free gum, and time usually help
- Jitteriness or feeling overstimulated: sometimes improved by a slower titration
- Headache or nausea: often temporary during startup
- Increased anxiety: more likely if the dose rises too fast or baseline anxiety is already high
This is one of the trade-offs with Wellbutrin. A medication that can help with drive and initiation may feel activating before it feels settling. I tell patients to picture it less as a sedating blanket and more as a morning light switch. For the right person, that is helpful. For the wrong person, or at the wrong dose, it can feel too bright.
A practical comparison helps:
| Concern | Wellbutrin (Bupropion) | Typical SSRIs (e.g., Prozac, Zoloft) |
|---|---|---|
| Main neurotransmitters targeted | Dopamine and norepinephrine | Serotonin |
| Energy profile | Often more activating | May feel more calming or sedating for some people |
| Sexual side effects | Often less troublesome for many patients | More commonly reported in practice |
| Weight changes | Significant weight gain is less commonly a reason people stop it | Weight changes are discussed more often |
| Best symptom fit | Low energy, low motivation, poor initiation | Anxiety, rumination, emotional reactivity may guide selection in some cases |
Serious safety issues
The biggest safety issue with Wellbutrin is seizure risk. That risk is still low at standard prescribing ranges, but low does not mean irrelevant. It matters more if a patient has a seizure history, active alcohol misuse, an eating disorder history, or other factors that lower seizure threshold. This is why prescribers increase the dose carefully and ask direct questions that may seem unrelated at first.
Blood pressure also deserves attention. Some patients notice an increase, especially if they already have hypertension or are combining Wellbutrin with other activating substances. Agitation, rash, allergic symptoms, or a sharp change from expected startup effects should prompt a message to your clinician right away.
Telepsychiatry works well for this part of treatment because follow-up can be specific and timely. We can adjust dose timing, slow a titration, or reconsider whether the formulation fits before frustration turns into abrupt stopping.
A few rules prevent many avoidable problems:
- Take it exactly as prescribed. Do not double a missed dose unless your prescriber tells you to.
- Use morning dosing if sleep becomes an issue. Late dosing often makes insomnia worse.
- Be honest about your history. Seizures, eating disorders, alcohol use, and substance use all affect safety.
- Report activation early. Restlessness, panic, irritability, or reduced sleep are easier to address early than after a difficult week.
- Do not crush or split tablets unless your prescriber says it is safe. Release mechanism matters.
Good treatment is not just choosing the medication. It is choosing the right version, at the right pace, with enough follow-up to handle the trade-offs well.
Wellbutrin in Your Integrative Telepsychiatry Plan
Medication works best when it creates traction for the rest of treatment. That idea is especially important with Wellbutrin because its benefits often show up in energy, focus, and willingness to engage.
Medication is one tool, not the whole plan
A person who starts getting out of bed more easily may finally have enough activation to attend therapy consistently, restart exercise, or prepare real meals instead of relying on convenience foods. In that sense, Wellbutrin can be a bridge. It doesn't replace psychotherapy, movement, sleep hygiene, or nutrition. It can make those interventions more reachable.
That’s one reason some patients benefit from a broader approach to holistic depression treatment. When a medication supports drive without commonly causing the weight gain or sexual side effects that push some people away from treatment, it can fit more naturally into long-term recovery work.

Why telepsychiatry works well for this medication
Telepsychiatry can be a strong format for Wellbutrin follow-up because the first weeks often require observation more than complexity. The important questions are concrete. Is sleep worse or better. Is the patient more activated or too activated. Is appetite changing. Is there enough momentum to build structure around the early response.
That kind of monitoring often works very well by secure video and patient portal communication. Patients in Pennsylvania don't have to lose half a day commuting just to report that they’re sleeping less, feeling more alert, or noticing the first signs of improved task initiation.
A medication plan is stronger when follow-up is easy. Convenience isn't just a comfort issue. It directly affects consistency, reporting, and treatment adjustment.
An integrative approach also changes how progress is judged. Success isn't only “less depressed.” It may also mean walking three times a week again, focusing through work meetings, reducing nicotine dependence, or having enough motivation to use therapy skills in real time. Wellbutrin often makes the most sense when care is organized around those real-life outcomes.
Frequently Asked Questions About Wellbutrin
Can alcohol be used with Wellbutrin
Caution is important. Wellbutrin can lower seizure threshold, so alcohol use matters, especially heavy use or abrupt changes in drinking patterns. Patients should discuss their actual alcohol intake fully with their prescriber rather than assuming occasional or social drinking is always irrelevant.
What should someone do if a dose is missed
In general, the safest principle is not to double the next dose. Taking doses too close together can increase side effect burden and may increase seizure risk. The exact instruction depends on the formulation and how much time has passed, so patients should follow the directions given for their prescribed version.
Can Wellbutrin make anxiety worse
Yes, it can for some people. Because it tends to be more activating, a person who is already physically tense, panicky, or highly sensitive to stimulation may feel more jittery at the start. That doesn't happen to everyone, but it is one of the clearest trade-offs with this medication.
Is Wellbutrin a stimulant
No. It affects dopamine and norepinephrine, but it isn't classified as a stimulant. That matters because some patients expect an immediate stimulant-like effect and are disappointed or confused when the experience is steadier and more gradual.
How is it different from stimulant treatment for ADHD
Stimulants are often more direct and more potent for core ADHD symptoms. Wellbutrin may still be useful when depression and attention problems overlap, or when a non-stimulant path is preferred. The decision usually depends on whether the main target is mood, focus, or both.
Does Wellbutrin usually cause weight gain
Significant weight gain is generally considered uncommon with this medication. That’s one reason it often stands out in antidepressant discussions. Still, appetite and weight experiences vary from person to person, so clinicians look at the whole pattern rather than assuming one universal response.
The right question isn't “Is Wellbutrin good or bad?” It's “Is this mechanism a good fit for this person's symptoms, risks, and goals?”
Partnering For Your Mental Wellness Journey
Wellbutrin is easiest to understand when viewed as a targeted tool. It works by helping dopamine and norepinephrine stay active longer, which can support energy, motivation, focus, and re-engagement with life. For many adults, that makes it meaningfully different from serotonin-first antidepressants.
The larger point is that medication works best in partnership with a broader plan. When patients understand the timeline, expect the trade-offs, and use early gains to support therapy, exercise, routine, and nutrition, treatment becomes more effective and more sustainable. People who want more context on collaborative care can also benefit from reading practical health guides for patients, especially when they’re trying to make informed choices about long-term mental health treatment.
If low energy, poor motivation, depression, focus problems, or nicotine dependence have been affecting daily life in Pennsylvania, Integrative Psychiatry of America offers secure online care with board-certified psychiatric nurse practitioners who build personalized treatment plans around medication, therapy, nutrition, exercise, and other whole-person supports.

