
A resident in Philadelphia finishes work, sits down, and notices the same pattern again. The body is tense for no clear reason. Sleep feels shallow. Loud sounds hit too hard. Driving past a certain block in Pittsburgh, Harrisburg, or Lancaster can bring back a wave of panic, even when life on paper looks fine. Another person in Erie or Scranton may not call it PTSD yet, but they know something isn't settling. They avoid reminders, stay on guard, and feel exhausted by how much effort it takes to get through ordinary days.
That experience is common in trauma care. PTSD doesn't always look dramatic from the outside. Sometimes it looks like irritability, isolation, poor sleep, relationship strain, trouble concentrating, or feeling emotionally numb. Many adults in Pennsylvania spend months or years trying to manage it alone before searching for real help.
Effective PTSD treatment options do exist, and they're more accessible than many people realize. Trauma-focused therapy, medication management, specialized interventions, and whole-person strategies can all play a role. For people who want care from home, telepsychiatry also makes it possible to start treatment without a long commute across Pennsylvania.
Table of Contents
- The First Step Toward Healing From PTSD
- Trauma-Focused Psychotherapy The Gold Standard
- Medication Management for PTSD Symptoms
- Emerging and Specialized PTSD Treatments
- The Power of an Integrative and Lifestyle Approach
- Accessing PTSD Care Through Telehealth in Pennsylvania
- How to Choose Your Path to Recovery
The First Step Toward Healing From PTSD
The first step is often smaller than people expect. It may be admitting that the nervous system hasn't come back down after something overwhelming, violent, frightening, or destabilizing. It may be realizing that the problem isn't a lack of willpower. It's that the brain and body are still reacting as if danger is present.
A person in Reading may keep replaying a crash. A healthcare worker in Philadelphia may feel detached after repeated traumatic events on the job. A veteran in Pittsburgh may avoid sleep because nightmares keep returning. A survivor of assault in Allentown may feel jumpy in crowds and ashamed that “it should be over by now.” These are different stories, but the clinical pattern is familiar.
PTSD treatment starts with accurate assessment and a plan that fits the person, not a generic checklist. That usually means looking at symptoms, trauma history, sleep, mood, substance use, daily functioning, medical factors, and what kinds of treatment feel realistic right now. Someone who can't tolerate exposure-based work on day one still deserves a legitimate path forward.
Signs that it's time to seek help
- Daily life keeps shrinking: work, driving, social plans, or sleep routines are getting organized around avoidance.
- The body won't power down: hypervigilance, startling easily, muscle tension, and poor sleep keep repeating.
- Memories feel current instead of past: reminders trigger a strong physical or emotional response.
- Other symptoms are piling on: depression, panic, irritability, or concentration problems are making recovery harder.
PTSD often convinces people to wait until things get worse. Early care usually gives more room to work.
For people trying to sort out whether they're dealing with trauma symptoms, panic, or generalized anxiety, reputable psychoeducation can help. These evidence-based anxiety resources give patients a clearer starting point before a clinical evaluation.
Trauma care also works best when the setting feels safe and structured. A trauma-informed mental health care approach matters because pacing, collaboration, and nervous-system regulation shape whether treatment feels manageable or overwhelming.
Trauma-Focused Psychotherapy The Gold Standard
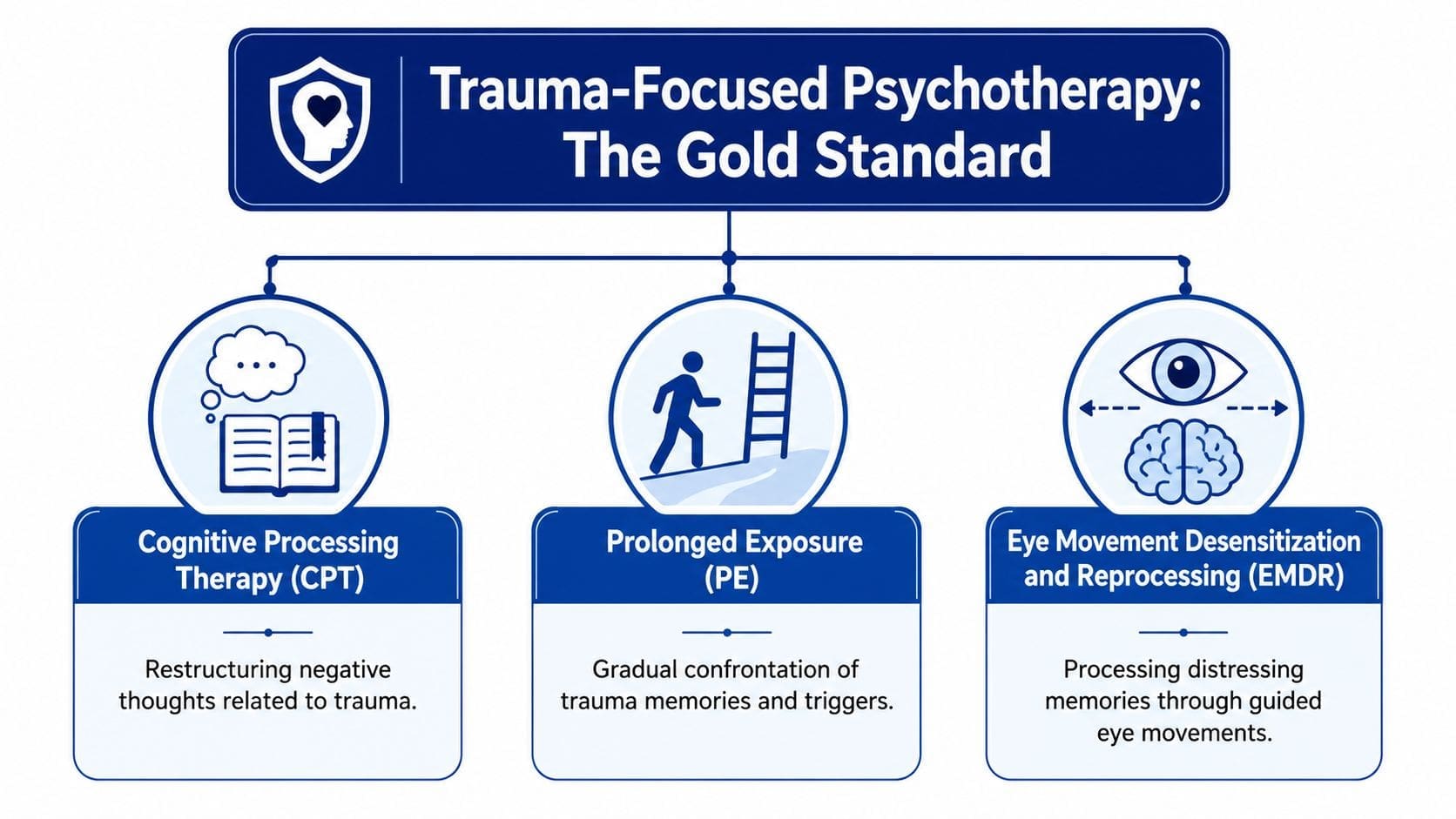
For most adults with PTSD, the strongest starting point is trauma-focused psychotherapy. The main evidence-based approaches are Cognitive Processing Therapy or CPT, Prolonged Exposure or PE, and Eye Movement Desensitization and Reprocessing or EMDR. The names can sound technical, but the core purpose is simple. These treatments help the brain stop treating the trauma as if it's still happening now.
What these therapies actually feel like
CPT focuses on the meanings attached to trauma. Many patients carry beliefs like “I'm not safe anywhere,” “It was my fault,” or “I should have done something different.” CPT helps identify those stuck points and test them against reality. It often feels structured and practical, especially for adults who want language, worksheets, and clear cognitive tools.
PE works through avoidance. The brain learns fear partly by pairing memories, places, sensations, and situations with danger. PE helps patients approach trauma memories and triggers gradually, with support, so the nervous system can relearn that the threat is not happening in the present. It isn't about forcing someone into distress. It's about careful repetition with a plan.
EMDR helps patients process distressing memories while using guided bilateral stimulation, such as eye movements. Many patients experience EMDR as less verbal than CPT. It can be a good fit for people who struggle to explain everything in detail but still want to process what happened.
A simple way to think about these three options:
| Treatment | Best described as | Often helpful for |
|---|---|---|
| CPT | examining trauma-related beliefs | guilt, shame, self-blame |
| PE | reducing avoidance through gradual exposure | fear, avoidance, trauma triggers |
| EMDR | reprocessing distressing memories | vivid traumatic recall, emotionally charged memories |
Why experts prioritize these treatments
The clinical hierarchy is clear. The VA/DoD overview of PTSD therapy explicitly recommends Prolonged Exposure, Cognitive Processing Therapy, and EMDR as the most effective treatments for PTSD, and it prioritizes individual trauma-focused psychotherapy over medication.
That recommendation matches outcome data. According to the Anxiety and Depression Association of America treatment facts page, 53 out of 100 patients who complete CPT, PE, or EMDR will no longer meet diagnostic criteria for PTSD, compared with 42 out of 100 treated with medication alone.
A review in Dialogues in Clinical Neuroscience describes trauma-focused manualized psychotherapies, specifically CPT, PE, and EMDR, as the gold-standard first-line interventions for PTSD, with strong evidence supporting 12 to 20 weekly 60-minute sessions.
Practical rule: the best therapy for PTSD is usually the one a patient can engage with consistently, complete at an adequate dose, and tolerate without shutting down.
Patients in Pennsylvania who want these approaches through telehealth often look for a provider familiar with structured trauma care. A directory of PTSD therapists and treatment support can help narrow that search.
Medication Management for PTSD Symptoms
Medication isn't a replacement for trauma treatment, but it can be a major part of a functioning treatment plan. For some patients, medication reduces the intensity of symptoms enough to make therapy possible. For others, it helps with the overlapping problems that PTSD often drags in, such as anxiety, depressive symptoms, sleep disruption, and constant physiologic arousal.

What medication can help with
The goal of medication management is usually symptom reduction, not erasing the trauma itself. In practice, that means targeting the symptoms that keep someone stuck. Intrusive thoughts, constant tension, low mood, panic symptoms, poor sleep, and emotional reactivity may all become easier to manage when the right medication is used carefully.
The evidence supports medication as a legitimate treatment pathway. PTSD statistics summarized by The Recovery Village report that psychotherapy can lead to improvement in as many as 46% of individuals within six weeks, while approximately 62% of patients receiving medication for PTSD also achieve significant improvement.
That doesn't mean every patient should start with medication. It means medication should not be dismissed, especially when symptoms are severe enough to interfere with work, parenting, therapy participation, or sleep.
Common medication decisions in PTSD often involve questions like these:
- Is anxiety so high that therapy feels impossible right now
- Is sleep disruption worsening everything else
- Are depression symptoms reducing motivation and daily functioning
- Have previous medications helped or caused side effects
Medication often works best when it creates enough stability for the patient to do the deeper work of recovery.
What good medication management looks like online
Good prescribing is never just “try this and check back in six months.” It starts with a full psychiatric evaluation, including trauma symptoms, other diagnoses, past medication responses, medical history, sleep, and safety concerns. Follow-up visits matter because PTSD symptoms change over time, and side effects can shape adherence just as much as effectiveness.
A strong virtual process usually includes:
- Initial evaluation: symptom review, diagnosis, treatment goals, and medication history.
- Medication selection: choosing a medication based on the symptom pattern and risk profile.
- Monitoring: tracking benefit, side effects, sleep, mood, and day-to-day function.
- Adjustment: changing dose, changing medication, or combining medication with therapy and lifestyle strategies.
In Pennsylvania, this can be done through secure telehealth for many adults. Online medication management appointments make it easier for patients in Philadelphia, Pittsburgh, Scranton, or rural parts of the state to get consistent follow-up without repeated travel.
Emerging and Specialized PTSD Treatments
Not every patient can step directly into standard trauma-focused therapy. Some become overwhelmed by exposure work. Some have co-occurring neurological issues. Others have persistent symptoms after trying more familiar PTSD treatment options. That's where specialized care becomes important.
When standard treatment is hard to tolerate
One of the most clinically important examples involves patients with both PTSD and traumatic brain injury or TBI. For these individuals, traditional trauma processing may be too activating, too cognitively taxing, or not the right fit at the start.
The STRONG STAR non-trauma intervention summary describes an 8-session non-trauma intervention that focuses on symptom tracking, stress management, relaxation, biofeedback, and cognitive strategies. It has been shown to significantly reduce PTSD symptoms without requiring direct trauma exposure. That matters for veterans, first responders, and others who can't tolerate standard exposure-based work.
This type of treatment reflects a useful clinical principle. A patient doesn't need to start by reliving the worst moment of their life to begin getting better. Sometimes the right entry point is regulation first, trauma processing later.
Where newer treatments may fit
Some interventions sit outside standard first-line care but still deserve discussion in a modern treatment plan.
- TMS: transcranial magnetic stimulation is a noninvasive brain stimulation treatment already used in other psychiatric settings. The current VA/DoD guideline acknowledges insufficient evidence for PTSD, but there's ongoing clinical interest in it for selected patients.
- Ketamine: ketamine is being explored for treatment-resistant PTSD, especially when mood symptoms are also significant. Evidence is still evolving, and it requires careful screening and monitoring.
- Stellate ganglion block: this procedure aims to reduce sympathetic overactivation. Some patients seek it when hyperarousal remains intense despite standard care.
These options are not the first move for most patients. They're better understood as next-step or specialized tools when the usual path hasn't provided enough relief, or when symptom patterns suggest another route may help.
For adults in southeastern Pennsylvania exploring this category, ketamine treatment information in Philadelphia is one example of how specialized services may fit into a broader psychiatric plan.
The Power of an Integrative and Lifestyle Approach
A patient may finish a strong therapy session, log off, and still spend the night sleeping lightly, skipping meals, bracing at every sound, and relying on caffeine to push through work the next day. That pattern matters. PTSD symptoms rise and fall in daily life, so treatment works better when the plan addresses daily life directly.
Lifestyle care is part of treatment, not a side note
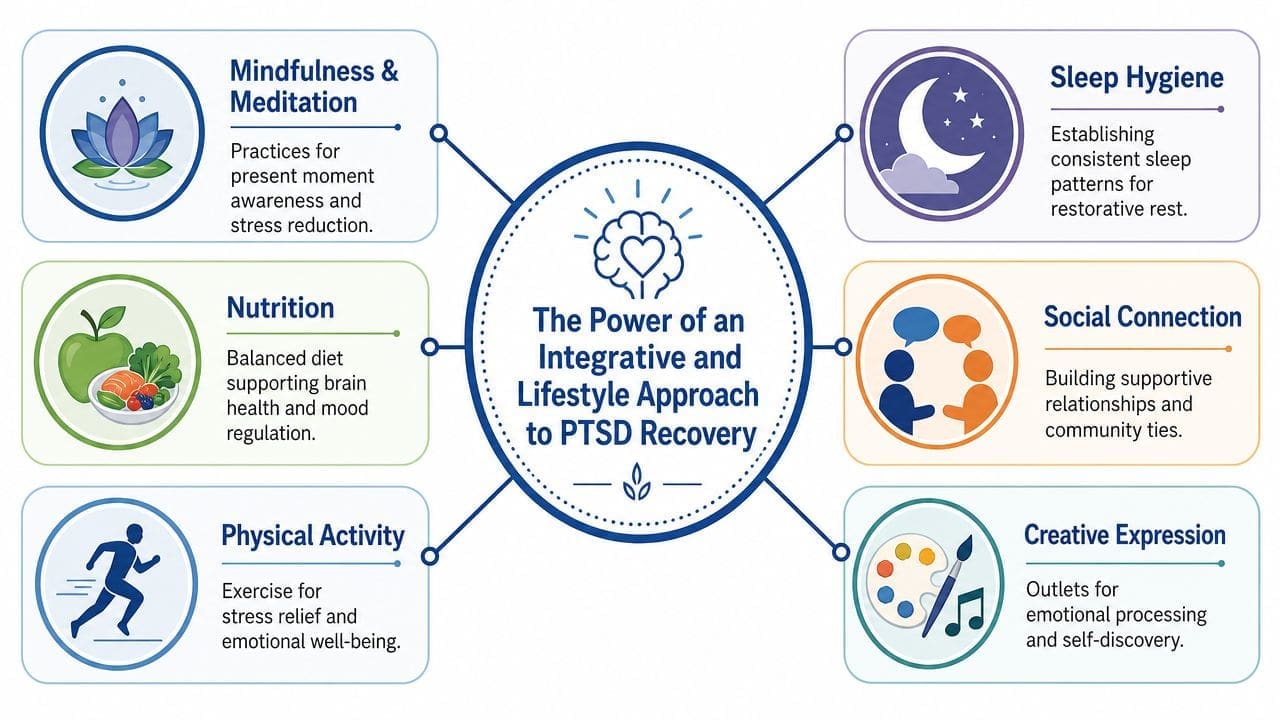
Lifestyle strategies are not generic add-ons. They target the same systems PTSD disrupts: arousal, sleep, concentration, body tension, mood stability, and the sense of safety in the present moment.
In practice, I see better follow-through when patients understand the trade-off. Therapy can help process trauma. Medication can reduce symptom intensity. But if sleep stays chaotic, alcohol becomes a nightly coping tool, or the body remains in a constant state of activation, progress is often slower and less stable. A whole-person plan gives patients more than symptom insight. It gives them a way to reduce the number of times the nervous system gets pushed back into overload.
Several daily areas deserve direct attention:
- Sleep hygiene: regular sleep and wake times, less stimulation before bed, and direct treatment for insomnia or nightmares when they are present.
- Exercise: steady movement can lower physical tension and improve regulation. Patients who want structure may benefit from an Exercise Routine Generator.
- Mindfulness and grounding: present-focused skills can help separate a trauma reminder from immediate danger.
- Nutrition: irregular meals, heavy alcohol use, and too much caffeine can worsen irritability, anxiety, and sleep disruption. Patients who want a deeper look at the brain-body connection can review how nutrition affects mental health.
- Connection and routine: isolation often strengthens PTSD symptoms. Predictable contact with supportive people and a repeatable daily structure can reduce drift and withdrawal.
Practical tools patients can use between visits
The best plans are concrete. Patients do better when they have specific tools to use on a Tuesday afternoon, not just ideas discussed during an appointment.
A few useful examples include:
- Mood tracking: a Feeling Journal can help identify triggers, body cues, and patterns that might otherwise get missed.
- Grounding during activation: the 5-4-3-2-1 Grounding Tool gives patients a structured way to come back to the present when symptoms spike.
A treatment plan is stronger when the patient knows what to do between appointments, not just during them.
One Pennsylvania-based telepsychiatry option, Integrative Psychiatry of America, combines virtual psychiatric evaluation, medication management, and evidence-informed mental health treatment with lifestyle and integrative support. That model fits adults who want PTSD care that addresses symptoms, physical regulation, and day-to-day functioning.
Accessing PTSD Care Through Telehealth in Pennsylvania
For many adults, access is the main obstacle. A patient in Philadelphia may struggle to fit weekly care around work. Someone in Erie may not live near a trauma-focused provider. A parent in Lancaster may need care during school hours without losing half a day to driving. Telehealth changes that equation.
Virtual PTSD care can work well for evaluation, medication management, follow-up, psychoeducation, symptom monitoring, and many therapy-based services. Patients in Pittsburgh, Allentown, Reading, Harrisburg, Scranton, and smaller communities across Pennsylvania often prefer it because it reduces travel, scheduling friction, and the stress of sitting in a waiting room when symptoms are already high.
How virtual PTSD care usually works
The first appointment usually focuses on assessment. The clinician reviews symptoms, trauma history, medical factors, treatment history, safety, and goals. From there, the plan may include therapy referral, medication, structured follow-up, and practical tools for symptom tracking or grounding.
What patients usually need is straightforward:
- A private space: headphones help if home privacy is limited.
- A reliable device: phone, tablet, or laptop with camera access.
- A plan for follow-up: regular visits matter more than perfect motivation.
Some patients want a visual sense of what online care looks like before booking. This short overview helps make that format more concrete.
Questions to ask before booking
A good fit matters in telepsychiatry just as much as in-person care. Before scheduling, patients should ask:
- Does the practice treat PTSD regularly: trauma care requires specific clinical experience.
- Can the practice provide statewide telepsychiatry in Pennsylvania: this matters if the patient lives outside Philadelphia.
- What services are offered virtually: evaluation, medication management, therapy coordination, and follow-up should be clear.
- How are refills and messages handled: a usable patient portal makes ongoing care much smoother.
The best virtual care doesn't feel distant. It feels organized, responsive, and easier to maintain.
How to Choose Your Path to Recovery
The best PTSD treatment options are the ones that match the actual clinical picture. A patient with strong avoidance and trauma-related beliefs may benefit most from trauma-focused therapy. A patient who can't sleep, can't function at work, and can't tolerate therapy intensity may need medication and nervous-system stabilization first. A patient with TBI or a history of shutting down in exposure work may need a different entry point.
That's why PTSD care should be collaborative. The right question isn't “What is the one best treatment for everyone?” The right question is “What combination is most likely to help this person move safely and steadily toward recovery?”
A useful way to think about the decision:
| Situation | Often worth considering |
|---|---|
| Ready to address the trauma directly | CPT, PE, or EMDR |
| Too symptomatic to engage fully in therapy | medication management plus supportive skills |
| Complex presentation or poor tolerance for exposure | specialized or non-trauma approaches |
| Recovery keeps stalling between visits | stronger lifestyle structure and tracking tools |
Patients don't need to have every answer before reaching out. They only need a starting point. For some, that's scheduling a confidential evaluation. For others, it's verifying insurance, using a grounding tool, or beginning to track symptoms more clearly so the first appointment is more productive.
Pennsylvania residents who want virtual, evidence-informed psychiatric care can learn more through Integrative Psychiatry of America. The practice offers telepsychiatry across the state, including support for PTSD, medication management, and whole-person treatment planning. Patients can review services, verify insurance coverage, schedule an appointment, or use free tools such as the Adult ADHD Assessment, Anxiety Symptom Checker, and Daily Agenda Planner.

