A positive pregnancy test can make an ordinary morning feel instantly complicated. For many adults with ADHD, the first thought isn't only about the pregnancy itself. It's also, "Can you take Vyvanse while you're pregnant?" and "Did taking it before this moment already cause harm?"
That question deserves a calm, careful answer. Vyvanse can be essential for daily functioning, but pregnancy changes how every medication decision is weighed. The safest next step usually isn't stopping suddenly on your own. It's talking through the full picture with a prescribing clinician and your obstetric team, especially if ADHD symptoms affect driving, work performance, appointment follow-through, meals, or emotional regulation.
Table of Contents
- The Moment You See a Positive Test
- What Vyvanse Does for ADHD Management
- Reviewing the Evidence on Vyvanse and Pregnancy Risks
- The Overlooked Risks of Untreated ADHD During Pregnancy
- Creating Your Personalized Pregnancy Plan for ADHD
- Guidance for Pre-Conception, Breastfeeding, and Postpartum
The Moment You See a Positive Test
Some patients have spent years finally getting their ADHD symptoms under control. They know what happens without treatment. Bills go unpaid, meals get skipped, sleep becomes chaotic, emotions run hot, and work becomes harder to hold together. Then a pregnancy test turns positive, and the medication that helped life feel manageable suddenly feels uncertain.
That uncertainty is real. It often shows up as guilt, panic, and urgency all at once. Some patients search online and find alarming summaries without context. Others assume they have to stop immediately, even if they have moderate or severe impairment when untreated.
What usually matters first
The first few questions are practical, not philosophical:
- How severe are the ADHD symptoms without medication? Some people can function with structure and therapy alone. Others can't safely do that.
- How far along is the pregnancy? Timing matters when reviewing exposure and planning next steps.
- What else is going on? Blood pressure history, sleep problems, anxiety, depression, appetite, and work demands all affect the decision.
- Who is coordinating care? A psychiatric prescriber and obstetric clinician should be looking at the same picture.
A rushed decision made from fear isn't the same as a thoughtful decision made from evidence.
Some patients need urgent medication guidance because their job requires sustained concentration or their symptoms make everyday tasks unsafe. Others may have enough support and symptom control to consider tapering. Both situations are common. Neither means someone is doing pregnancy the wrong way.
When symptoms have been impairing for years, a mental health evaluation isn't optional. This guide on when to see a psychiatric prescriber for ADHD and related concerns can help clarify when a medication conversation should happen right away.
What Vyvanse Does for ADHD Management
Vyvanse is the brand name for lisdexamfetamine, a stimulant medication used for adult ADHD treatment. In practice, patients don't take it because they want to feel stimulated. They take it because it can improve attention, task initiation, follow-through, impulse control, and the ability to organize daily life.
For many adults, that changes far more than work output. It affects whether prenatal vitamins are remembered, whether meals happen on time, whether driving stays focused, and whether a day has enough structure to feel survivable.
Why stopping isn't a neutral choice
When Vyvanse is working well, patients often describe fewer dropped tasks and less mental noise. They may also notice steadier emotional responses and less friction around transitions. Those benefits matter during pregnancy because pregnancy asks for more planning, not less.
A medication decision should be made in the context of what the medication is doing. This overview of ADHD medication options is useful for understanding where stimulants like lisdexamfetamine fit in a broader treatment plan.
What works and what doesn't
A few patterns come up again and again in clinical care:
| Approach | What tends to happen |
|---|---|
| Stopping suddenly without a plan | Patients may feel overwhelmed, disorganized, irritable, or unable to keep routines in place |
| Reducing external demands while adding support | Some patients can manage with therapy, sleep structure, reminders, and family help |
| Using the lowest effective medication strategy when needed | Often the most realistic option when ADHD symptoms are impairing safety or functioning |
Non-medication support helps, but it doesn't replace stimulant benefit for everyone. Sleep hygiene, calendar systems, meal planning, movement, and psychotherapy can make a major difference. They just aren't identical to medication.
Access can also complicate treatment. If a patient is already dealing with pharmacy disruptions, this practical guide on navigating Adderall and Vyvanse shortages can help frame conversations about continuity and substitution.
Reviewing the Evidence on Vyvanse and Pregnancy Risks
A positive pregnancy test often creates pressure to make a fast decision. In practice, this decision is usually better when it is slowed down enough to ask the right questions. How severe are the ADHD symptoms off medication? What happened in prior pregnancies, if applicable? Are there blood pressure concerns, appetite issues, or a history of preterm birth that change the risk picture?
What the research supports, and what it does not
Vyvanse is lisdexamfetamine, a stimulant in the amphetamine family. That matters because pregnancy discussions about stimulants usually focus on three categories of risk: birth defects, pregnancy complications such as blood pressure or growth concerns, and newborn effects after delivery.
Those categories are not equally supported by the evidence.
A review from Integrative Psychiatry of America summarizes a 2023 cohort study in JAMA Psychiatry that looked at more than 5,000 stimulant-exposed pregnancies. In that review of Vyvanse safety in pregnancy, the reported findings were reassuring on major congenital malformations, with no significant increase detected, while still showing modestly higher risks for preterm delivery, low birth weight, and gestational hypertension.
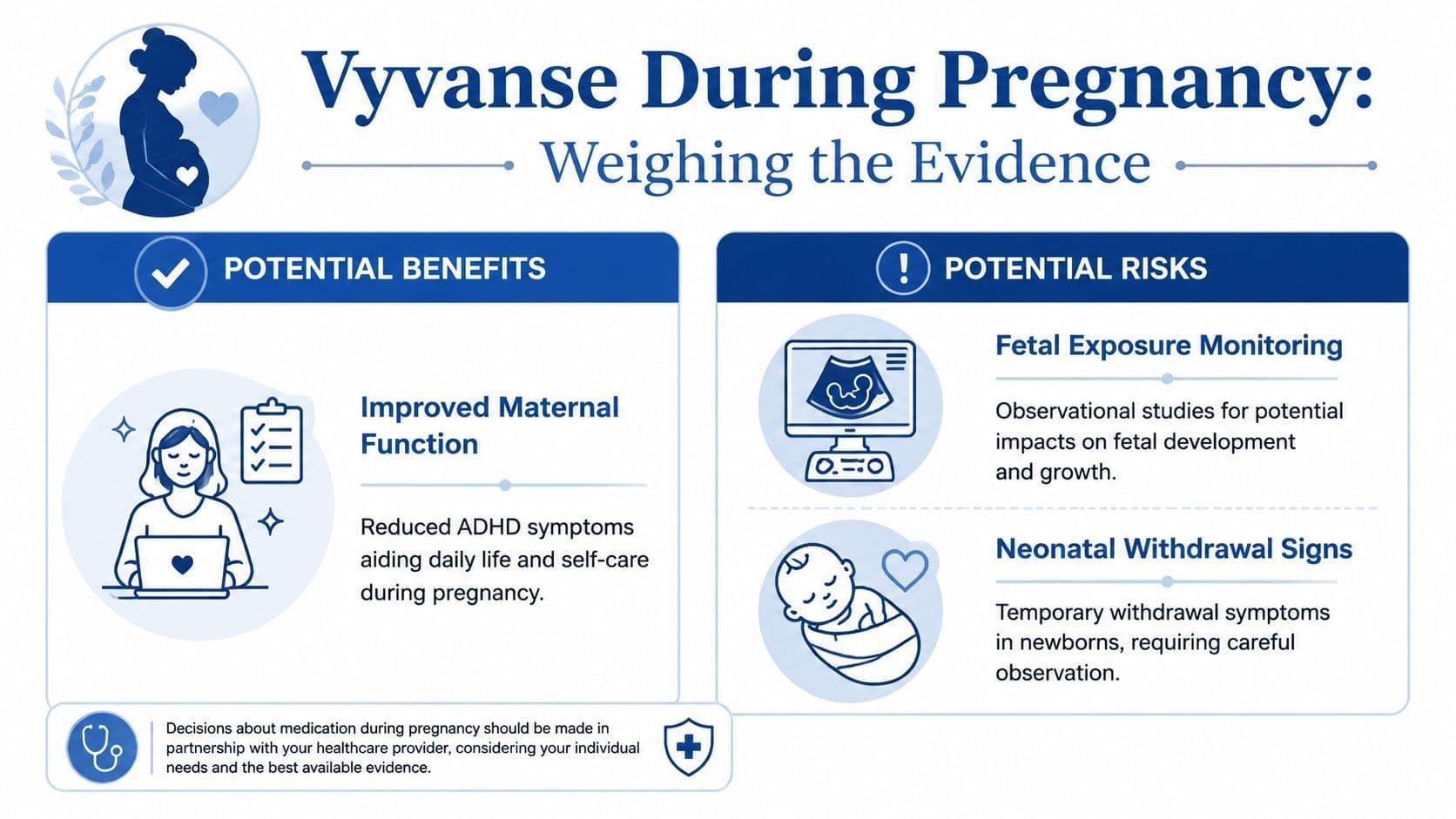
That is often the conversation I have with patients. The biggest fear is usually, "Did I already harm the baby?" Current evidence is more reassuring on major malformations than many patients expect. The harder part is deciding what to do with the smaller but still real concerns around pregnancy complications.
How to interpret that without oversimplifying it
No single study settles the question. Observational pregnancy data has limits, because patients who continue stimulants during pregnancy may differ from patients who stop them in ways that also affect outcomes. Severity of ADHD, smoking history, sleep, nutrition, stress, and coexisting psychiatric conditions can all matter.
So the practical takeaway is not "safe" or "unsafe."
The practical takeaway is that the evidence does not show a clear signal for major birth defects, but it does support careful attention to maternal blood pressure, fetal growth, appetite, weight, and timing of delivery if a stimulant is continued.
What this means in a real prescribing conversation
Shared decision-making works best when the medication question is tied to functioning, not fear alone. A patient with mild symptoms, strong home support, flexible work demands, and a history of doing well off stimulants may reasonably choose to taper off. A patient who becomes disorganized enough to miss medical appointments, stop eating regularly, drive unsafely, or spiral into anxiety after stopping may make a different choice.
Both decisions can be medically thoughtful.
I usually frame it this way:
- Major malformation risk looks more reassuring in newer large studies than many older online summaries suggest.
- Pregnancy complications still deserve monitoring, especially blood pressure, weight, and fetal growth.
- Symptom severity and functional impact should drive the plan, because the right answer depends on what happens when treatment is reduced or stopped.
For a broader review of ADHD medication during pregnancy, including stimulants and bupropion, this companion resource can help you compare options before making a plan with your prescriber and OB team.
The Overlooked Risks of Untreated ADHD During Pregnancy
Many online discussions focus so heavily on medication exposure that they leave out the condition being treated. That's a problem. Untreated ADHD in pregnancy can affect daily functioning in ways that are easy to underestimate until routines start falling apart.

A patient may stop Vyvanse with every good intention, then begin missing prenatal appointments, forgetting to eat regularly, driving while distracted, or losing the ability to manage work and home tasks. Another patient may become so overwhelmed that anxiety or depression worsens. Pregnancy doesn't erase executive dysfunction. It often amplifies the cost of it.
Where untreated symptoms cause friction
The risks don't always look dramatic at first. They often show up as repeated small failures in routine care.
- Missed appointments and delayed follow-up can happen when planning, time management, and reminders break down.
- Poor nutrition and hydration become more likely when grocery shopping, meal prep, and appetite cues are inconsistent.
- Safety issues matter if distractibility affects driving, medication management, or job performance.
- Relationship strain can increase when partners mistake symptoms for carelessness.
For women whose symptoms have been under-recognized for years, this discussion of ADHD in women and integrative treatments often helps put the emotional side of the diagnosis into context.
Sometimes the biggest pregnancy risk isn't the medication alone. It's the collapse in functioning that follows when severe ADHD is left untreated.
A short explanation can also help partners and family understand why this decision isn't simple:
The key trade-off
If ADHD symptoms are mild, stopping medication may be reasonable with added supports. If symptoms are severe, "just stop" can be poor medical advice. Shared decision-making works best when it respects both sides of the risk equation.
Creating Your Personalized Pregnancy Plan for ADHD
A positive pregnancy test often creates pressure to make a fast decision. In practice, the safest choice usually comes from slowing the moment down enough to ask better questions.
The plan starts with a clinical conversation, not a reflex. I want to know how you function on Vyvanse, what happened during past medication changes, whether your job or commute leaves little room for error, how your sleep and appetite are holding up, and who is available to help day to day. Those details matter more than a generic rule.
Three common paths
Some patients stay on Vyvanse during pregnancy. That choice is more common when ADHD symptoms are moderate to severe, prior attempts to stop led to major functional decline, or daily demands carry safety consequences. In those cases, treatment usually focuses on the lowest dose that still helps, regular blood pressure and appetite checks, and communication between psychiatric and obstetric care.
Others decide on a planned taper. That can be a reasonable option when symptoms are milder, home and work supports are reliable, and the patient feels prepared for some decrease in focus and productivity. A taper is usually easier than stopping abruptly because it gives us time to watch for sleep disruption, anxiety, irritability, or a drop in day-to-day functioning.
A third group uses a hybrid plan. That might mean reducing the dose, tightening behavioral supports, increasing therapy, changing work expectations for a season, or reconsidering whether medication is needed in each trimester. This is often the most realistic path because many patients do not fit neatly into a continue-or-stop decision.

What the plan should include regardless of the medication choice
Medication is only one part of keeping pregnancy stable with ADHD. The patients who tend to do best usually have a written, practical system around them.
Therapy with concrete ADHD tools
CBT-based work can help with planning, overwhelm, routine building, and the self-criticism that often flares when symptoms get worse.Food, hydration, and sleep structure
A plan for simple meals, water intake, and bedtime routines can protect functioning when appetite or energy becomes unpredictable. For added practical ideas, this guide to nutrition support during pregnancy with ADHD can help.Environmental supports that reduce mental load
Shared calendars, pharmacy auto-refills, pill organizers, reminder apps, duplicate chargers, and partner check-ins can prevent small mistakes from turning into bigger problems.Scheduled reassessment
The right plan at six weeks may not be the right plan at twenty-six weeks. Symptoms, nausea, appetite, blood pressure, and sleep can all change over the course of pregnancy, so follow-up should be built in from the start.
Earlier evidence review in this article covers what we know and what we still do not know about stimulant exposure in pregnancy. The practical takeaway for planning is straightforward. If medication is clinically necessary, the conversation shifts from "Is there any risk?" to "Which option creates the lowest overall risk for this patient right now?"
Whole-person planning matters
ADHD treatment during pregnancy also has to account for the ordinary physical problems that can throw off routines. Constipation, hemorrhoids, nausea, appetite changes, and body discomfort can make it harder to eat regularly, sleep well, and stay organized. For patients trying to make a realistic day-to-day plan, this guide on managing anorectal health while pregnant may be a helpful add-on to obstetric care.
One telehealth option for adults in Pennsylvania is Integrative Psychiatry of America, which provides ADHD medication management and integrative support such as psychotherapy, mindfulness, exercise counseling, nutrition education, and lab or genetic screening when clinically indicated.
Guidance for Pre-Conception, Breastfeeding, and Postpartum
A lot of women do not ask this question at the first positive test. They ask it months earlier, while trying to decide whether to conceive, whether to stay on medication, and how much disruption they can realistically absorb. That is the right time to start.
Pre-conception planning works best when it is specific. The goal is not to create a perfect pregnancy. The goal is to avoid rushed decisions later, when emotions are high and symptoms may already be harder to manage. In practice, I want to know what happened the last time medication was lowered or stopped, which symptoms caused the most impairment, and whether anxiety, depression, insomnia, or disordered eating also need attention before pregnancy.
I also want to know what daily life looks like. A patient with mild inattentiveness and strong support at home may have very different options from a patient whose untreated ADHD affects driving, work performance, medication adherence, or meal routines. Shared decision-making matters here because the same recommendation will not fit both people.
Lifestyle support is part of that planning, too. Regular meals, sleep structure, and realistic routines can make any medication plan work better. For patients who want practical ideas, this guide to nutrition during pregnancy for women with ADHD can help support consistency before and during pregnancy.
Before pregnancy
A good pre-conception visit usually covers a few practical questions:
- What happens when Vyvanse is reduced or stopped? Past experience often predicts how difficult a change may be.
- Are other symptoms affecting the picture? Anxiety, depression, insomnia, and appetite problems can shift the risk-benefit discussion.
- What support can be set up in advance? Therapy, partner involvement, reminders, work adjustments, and simplified routines all matter.
- Would pregnancy registry participation be a fit? Some patients want to contribute to what we learn about medication safety.
Breastfeeding requires a separate decision
Breastfeeding is a new risk-benefit conversation, not an automatic extension of the pregnancy plan. As noted earlier, Vyvanse and amphetamine exposure through breast milk raises concern for infant effects, so many clinicians advise against breastfeeding while taking it.
That guidance can feel discouraging, especially for women who already worked hard to make an informed pregnancy plan. It still does not mean there is only one acceptable path. Some patients decide that staying on the medication and using formula protects both maternal functioning and infant safety. Others want to discuss changing medications, pausing treatment, or using added non-medication supports during the breastfeeding period. The best choice depends on symptom severity, psychiatric history, feeding goals, and how realistic each option is in the first weeks after delivery.
Protecting the baby matters. Protecting the mother's ability to function safely matters, too.
Postpartum deserves its own monitoring plan
The postpartum period puts executive function under pressure fast. Sleep loss, feeding schedules, physical recovery, and mood changes can make previously manageable ADHD symptoms feel much more impairing.
A postpartum plan should be decided before delivery when possible, not only after problems show up. That plan often includes:
- A medication review soon after birth
- Mood monitoring for depression and anxiety symptoms
- Sleep protection where the household can realistically support it
- Clear task division at home so one parent is not carrying the invisible planning load
- Early follow-up if attention, irritability, or overwhelm start interfering with infant care or recovery
The broader question across pre-conception, breastfeeding, and postpartum is not whether one rule applies at every stage. It is which plan gives this mother the safest and most stable level of functioning at each stage, with room to reassess as her needs change.

