
Late at night, a person in Philadelphia, Pittsburgh, Harrisburg, or a small Pennsylvania town may be scrolling on a phone after another exhausting day, trying to understand why the same disturbing thought keeps showing up. The thought may feel violent, sexual, blasphemous, or plainly wrong. It may trigger panic, shame, and a desperate need to mentally “fix” it.
That search for intrusive thoughts OCD treatment usually comes from fear, not curiosity. People often worry that the thoughts mean something terrible about who they are. In many cases, they don't. Unwanted intrusive thoughts can be a symptom of obsessive-compulsive disorder, and OCD is a recognized medical condition with effective treatment options. Care can also be accessed privately from home through telehealth across Pennsylvania, which matters when leaving work, arranging transportation, or finding a local specialist feels like one more obstacle.
Table of Contents
- The Search for Relief from Unwanted Thoughts
- Understanding Intrusive Thoughts and the OCD Cycle
- The Gold Standard Treatment Exposure and Response Prevention
- Medication Management for OCD
- An Integrative Approach to Supporting Your Recovery
- Practical Coping Strategies for Difficult Moments
- How to Start OCD Treatment via Telehealth in Pennsylvania
The Search for Relief from Unwanted Thoughts
A common pattern looks like this. Someone in Scranton or Allentown has a thought they never wanted, such as “What if I lose control?” Then they check their reaction, replay the thought, ask for reassurance, avoid certain objects, or pray in a very specific way to feel safe again. Relief comes for a moment, then the thought returns stronger.
That cycle is frightening because it feels personal. It often convinces people that they must be dangerous, immoral, or broken. In OCD, the opposite is usually true. These thoughts are typically ego-dystonic, which means they clash with the person's values and feel intensely unwanted.
Why people often delay getting help
People in Lancaster, Reading, Erie, and throughout Pennsylvania often wait because of a few predictable concerns:
- Shame gets in the way. The content of the thought feels too upsetting to say out loud.
- People misread the symptom. They assume the thought reflects intent instead of anxiety.
- Access feels limited. Specialized OCD care may not be nearby.
- Schedules are tight. Parents, students, and professionals may struggle to attend in-person treatment consistently.
The thought itself isn't the best measure of risk. The person's relationship to the thought matters more.
For many adults, a significant turning point is learning that intrusive thoughts are a treatable symptom, not a hidden confession. Once that clicks, the question changes from “What kind of person thinks this?” to “What treatment helps?”
What relief usually requires
Effective care for OCD is usually specialized. General stress management alone often won't break the pattern. The most useful treatment plans focus on the actual OCD process, especially the fear-compulsion loop that keeps the symptoms alive.
Telehealth has made this much more realistic for people across Pennsylvania. Someone in Philadelphia may use it for convenience. Someone in a rural area may use it because there isn't an OCD-focused clinician nearby. In both cases, privacy, consistency, and easier follow-through can make treatment more accessible.
Understanding Intrusive Thoughts and the OCD Cycle
Some intrusive thoughts are part of normal human experience. A person may briefly imagine swerving off the road, shouting in a quiet room, or forgetting something important. Those thoughts can feel odd, but they usually pass.
Clinical intrusive thoughts are different because they stick, trigger intense distress, and pull a person into rituals meant to neutralize the fear.
When a thought is common and when it becomes clinical
About 80% of nonclinical samples report intrusive thoughts similar to clinical obsessions, but OCD requires significant distress or impairment in daily life, according to Pathlight's OCD statistics overview. That distinction matters. The presence of an upsetting thought alone doesn't automatically mean OCD.
A useful way to think about OCD is a faulty mental fire alarm. The brain sends a danger signal even when there isn't a real threat. The person then tries to get certainty, safety, or relief. That response makes sense emotionally, but it accidentally teaches the brain to keep sounding the alarm.
For readers who want another patient-friendly explanation of common OCD themes and how intrusive thoughts can present, Paramount Recovery Centers on OCD thoughts offers a helpful overview.
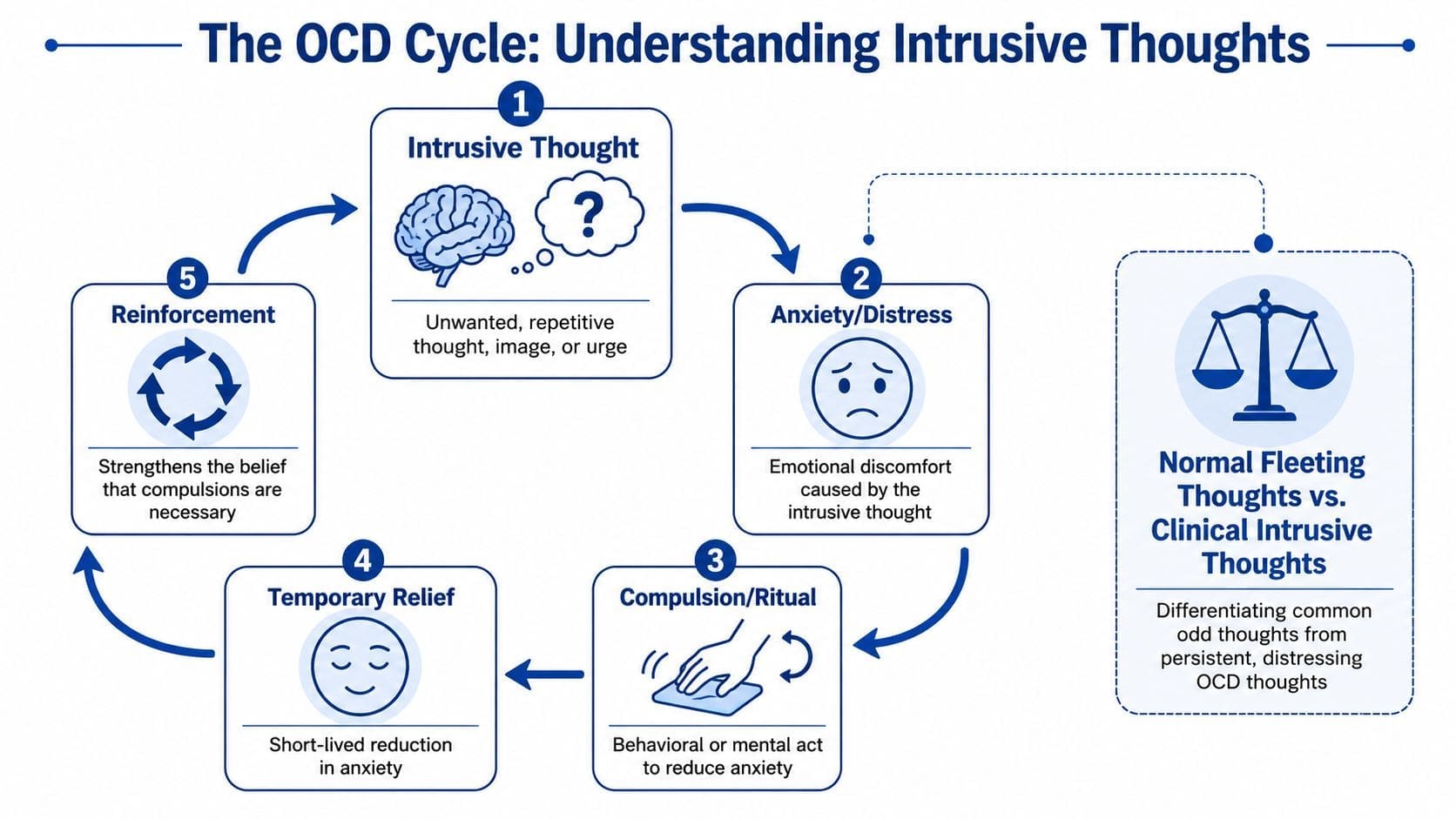
How the OCD loop keeps going
The cycle often follows the same sequence:
| Stage | What happens |
|---|---|
| Obsession | An unwanted thought, image, or urge appears |
| Anxiety | The person feels fear, disgust, guilt, or doubt |
| Compulsion | They check, avoid, reassure, review, confess, or repeat a ritual |
| Relief | Anxiety drops briefly |
| Reinforcement | The brain learns that the ritual must have “worked” |
Compulsions aren't always visible. Many people perform mental compulsions, such as reviewing memories, testing whether they feel “right,” replacing a bad thought with a good one, or scanning for certainty.
Clinical clue: If a thought keeps demanding reassurance, certainty, or ritualized relief, OCD moves higher on the list of possibilities.
That model often brings relief by itself. It explains why the thoughts feel so sticky and why trying harder to “solve” them usually backfires.
The Gold Standard Treatment Exposure and Response Prevention
Exposure and Response Prevention, usually called ERP, is the treatment most clinicians rely on when intrusive thoughts are part of OCD. It is not about forcing someone into extreme situations. It is a structured therapy that helps the brain stop treating the thought as an emergency.
ERP is the first-line and most effective treatment for OCD, with 65% to 80% of patients responding well, and research confirms ERP is as effective as, if not more effective than, medication for treating OCD in adults, according to the American Psychological Association's review of OCD diagnosis and treatment.
A short visual can make the process easier to understand.
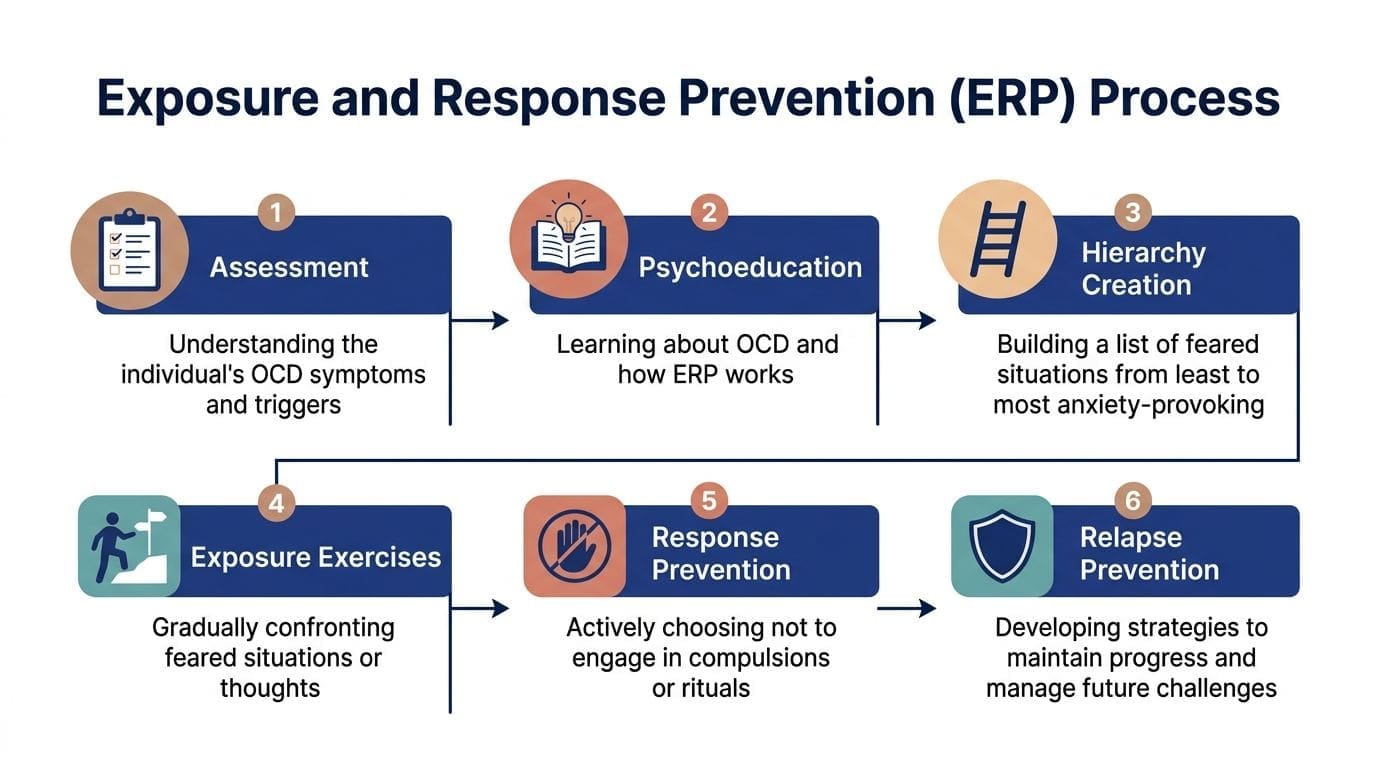
What ERP actually looks like
ERP has two parts.
Exposure means intentionally facing the thought, image, situation, or uncertainty that triggers OCD.
Response prevention means resisting the ritual that usually follows.
A simple example helps. If someone has contamination fears, an exposure might involve touching a doorknob and waiting before washing. If someone has harm obsessions, an exposure might involve writing the feared thought down and allowing the discomfort to rise without asking for reassurance or mentally canceling it.
ERP usually starts with a hierarchy, not the hardest item. The person and clinician build a ladder of triggers from easier to harder, then work upward.
- Lower-rung exposure: Read a word or sentence that triggers mild distress.
- Middle-rung exposure: Stay in a situation that usually prompts checking.
- Higher-rung exposure: Face a feared scenario while fully resisting rituals.
A related treatment overview on anxiety care in Pennsylvania through CBT, medication, and telepsychiatry can also help patients understand how structured therapy and medication support often fit together.
Later in treatment, many patients benefit from seeing ERP explained in action:
Why ERP works over time
ERP works because the brain can learn a new lesson. When a person experiences anxiety and doesn't perform the compulsion, the feared catastrophe usually doesn't happen. Over repeated practice, the alarm loses credibility.
This process is often called habituation or inhibitory learning, depending on the framework a clinician uses. Patients usually experience it more plainly as this: “The feeling rose, stayed uncomfortable for a while, then came down without the ritual.”
Recovery doesn't require proving the thought false. It requires learning that the thought doesn't need a ritualized response.
That's why reassurance-heavy approaches often stall progress. ERP asks a different question. Not “How can this thought be disproven?” but “How can a person live well even while uncertainty is present?” That shift is where real freedom tends to start.
Medication Management for OCD
Medication has an important role in intrusive thoughts OCD treatment, especially when symptoms are intense, time-consuming, or make therapy hard to tolerate. The main medication group used for OCD is Selective Serotonin Reuptake Inhibitors, or SSRIs.
Why SSRIs are used differently in OCD
OCD often requires a different medication strategy than depression. SSRIs are the primary medication class for OCD and are typically prescribed at doses double those used for depression. Research also confirms that a combination of high-dose SSRIs and ERP therapy yields superior outcomes compared with either treatment alone, as outlined in UT Southwestern's OCD treatment review.
That difference surprises many patients. Someone may have taken an SSRI years ago for depression or generalized anxiety and assume OCD treatment works the same way. Often it doesn't. OCD symptoms can be more stubborn and may need a higher therapeutic dose, more time, and closer follow-up.
For example, people starting sertraline often want to know when benefits might show up and why the timeline can feel slow. A practical breakdown is available in this guide on how long before Zoloft starts working.
What medication can and cannot do
Medication usually doesn't erase uncertainty. It tends to turn down the volume of the anxiety and urgency surrounding the obsession. That can make it easier to pause, resist rituals, sleep better, and participate in ERP with less overwhelm.
A realistic way to think about medication is:
- What it can do: Reduce symptom intensity, lower baseline anxiety, improve treatment participation.
- What it can't do alone: Teach the brain to stop relying on compulsions.
- What sometimes happens next: If SSRIs and ERP don't bring enough relief, clinicians may consider augmentation strategies or other advanced options based on symptom pattern and severity.
Medication is often most useful when it creates enough breathing room for therapy to work.
This is where careful prescribing matters. OCD treatment often requires patience, dose optimization, side-effect monitoring, and a plan that matches the person's symptoms rather than a one-size-fits-all approach.
An Integrative Approach to Supporting Your Recovery
The strongest OCD care plans usually combine evidence-based treatment with practical support for the body and nervous system. Lifestyle changes don't replace ERP or medication, but they can make hard treatment work more manageable.
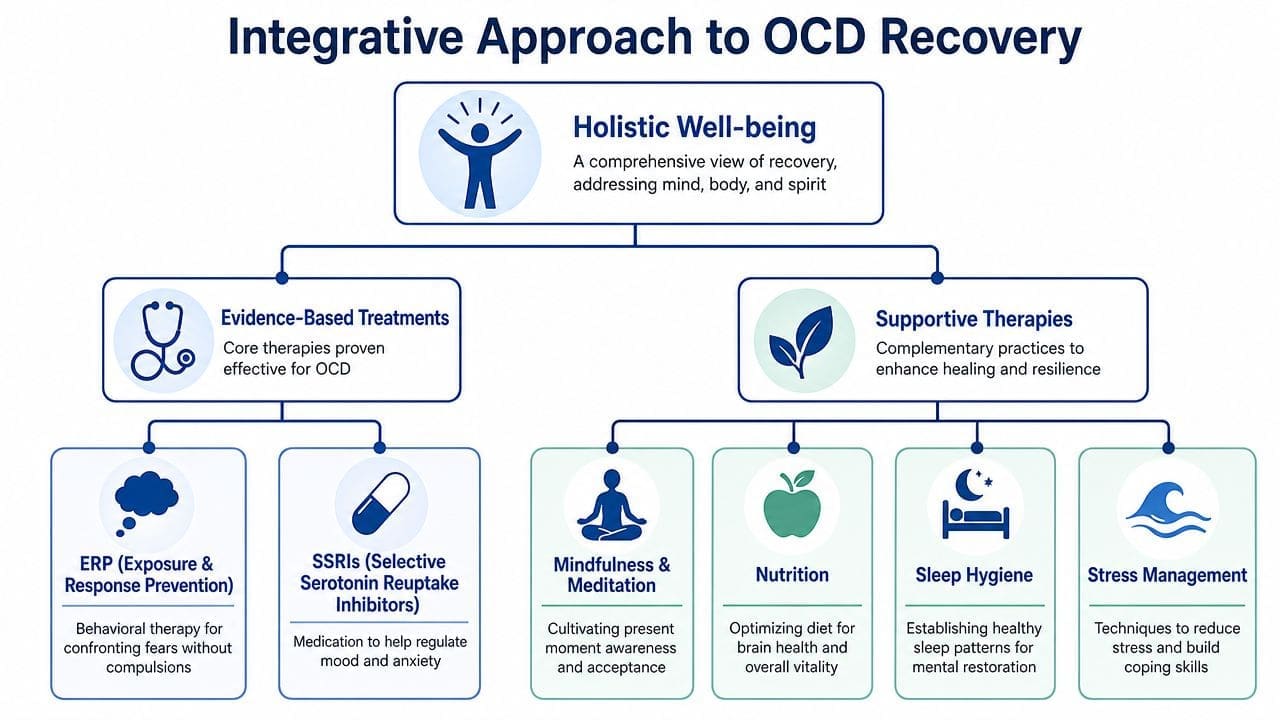
Lifestyle support that helps treatment stick
When sleep is poor, stress is high, and routines are chaotic, intrusive thoughts often feel louder. That doesn't mean lifestyle is the cause of OCD. It means the brain has fewer resources available for distress tolerance and follow-through.
Useful supports often include:
- Sleep consistency: Going to bed and waking up at regular times can reduce overall reactivity.
- Regular movement: Exercise won't cure OCD, but many patients notice it helps discharge tension and supports mood stability.
- Steady meals and hydration: Skipping meals can make anxiety feel sharper and more urgent.
- Mindfulness practice: The goal isn't to empty the mind. It's to observe thoughts without automatically obeying them.
Patients who want a broader overview of whole-person care can review integrative OCD treatment, which explains how medical and behavioral approaches can work together.
Useful tools between visits
The days between appointments matter. Small, repeatable practices often support more durable progress than occasional bursts of motivation.
A few practical tools can help:
- Track patterns with a journal. A brief log of triggers, rituals, and distress can make OCD patterns more visible. The Feeling Journal is one simple option.
- Reduce decision fatigue. A structured routine lowers the number of moments where anxiety can take over the day. The Daily Agenda Planner can help.
- Build sustainable movement. Exercise works better when the plan is realistic. The Exercise Routine Generator gives people a starting point.
This kind of support won't replace specialized care. It does help people show up to treatment with more stability, which often makes ERP practice and medication adherence easier.
Practical Coping Strategies for Difficult Moments
Long-term treatment changes the pattern. In the meantime, people still need something to do when the thought lands hard and the body reacts fast.
What to do when the thought hits
A better immediate response is usually simple, not dramatic.
- Label it clearly. Try mentally naming it: “This is an intrusive thought.” That creates a little distance between the person and the content.
- Allow discomfort to be present. Acceptance doesn't mean liking the thought. It means dropping the fight to make it disappear right now.
- Delay the ritual. If resisting completely feels too hard, waiting even a short time can weaken the automatic loop.
- Shift attention on purpose. Move toward a real task, a conversation, or a sensory grounding exercise instead of arguing with the thought.
- Use compassionate self-talk. Shame fuels OCD. A calmer stance often helps more than self-criticism.
A practical set of grounding skills is available in this guide to grounding techniques for anxiety, which can be especially useful during high-distress moments.
What usually makes it worse
Focused distraction and acceptance strategies are more effective for managing intrusive thoughts than thought suppression, which primarily exacerbates distress without reducing thought frequency. That principle was noted earlier in the medication discussion because the same source also addresses OCD treatment overall.
Trying not to think the thought often backfires. The brain starts monitoring for the thought, which keeps it active. That's why commands like “stop thinking that” or “prove you'd never do that” rarely help for long.
Useful reset: The goal isn't to win an argument with the thought. The goal is to stop feeding it with rituals, avoidance, and panic.
Many people also get trapped in online reassurance-seeking. Reading forum after forum to confirm “this means I'm safe” can subtly become another compulsion. A brief grounding exercise, a return to the present task, or planned ERP work usually helps more.
How to Start OCD Treatment via Telehealth in Pennsylvania
Getting evaluated for OCD doesn't have to mean long travel, time off work, or explaining sensitive symptoms in a crowded waiting room. For many adults in Pennsylvania, telehealth is the most practical way to start.
What the first steps usually look like
A good first appointment usually focuses on the actual symptom pattern. The clinician asks about the intrusive thoughts themselves, the compulsions that follow, how much time symptoms consume, what has already been tried, and whether medication, ERP referral, or both make sense.
Professional treatment is worth pursuing. Approximately 75% of people with OCD are significantly helped by CBT, with some services reporting recovery rates up to 80%, according to OCD UK's overview of cognitive behavioural therapy for OCD.
Patients who need prescribing support can also review options for online medication management, including how follow-up care is commonly handled through telehealth.
Why telehealth is a practical option statewide
Telehealth can work well whether someone lives in Philadelphia, Pittsburgh, Harrisburg, Erie, Scranton, Allentown, Lancaster, Reading, or elsewhere in the state. It offers privacy, easier scheduling, and broader access to clinicians who understand OCD rather than treating it like a generic anxiety problem.
A strong next step is simple:
- Schedule a confidential evaluation.
- Describe the thoughts and rituals fully, even if they feel embarrassing.
- Ask whether the plan includes ERP, medication management, or both.
- Follow through consistently enough to give treatment a fair trial.
People with OCD often wait too long because they're afraid of what the thoughts mean. Evidence-based care works best when the symptom is named clearly and treated directly.
If intrusive thoughts are interfering with daily life, Integrative Psychiatry of America provides virtual psychiatric evaluations, medication management, and evidence-informed mental health treatment throughout Pennsylvania. Adults across Philadelphia, Pittsburgh, Harrisburg, Erie, Scranton, Allentown, Lancaster, Reading, and statewide can explore confidential telehealth care from home. To take the next step, review treatment options, verify insurance coverage, schedule an appointment, or use one of the practice's free mental health tools to start building support today.

