
A positive pregnancy test can turn an ordinary morning into a cascade of urgent questions. For someone taking Vyvanse for ADHD, one of the first is often Can you take Vyvanse while you are pregnant? The honest answer isn't a simple yes or no.
What matters is the full clinical picture. Symptom severity, prior response to medication, blood pressure history, work demands, driving safety, anxiety, sleep, and pregnancy stage all affect the decision. Stopping suddenly may sound safer, but for some patients it creates its own risks, especially when ADHD symptoms are severe enough to disrupt daily functioning.
Older guidance often pushed people toward broad avoidance. That framework has changed. Vyvanse's active ingredient, lisdexamfetamine, was long treated under the FDA's older labeling system as pregnancy category C, which reflected animal risk data and limited human evidence rather than a clear conclusion of safety or harm. A review summarized in this discussion of Vyvanse in pregnancy also notes that ADHD medication use in pregnancy increased from 1998 through 2013, making this a common clinical issue rather than a rare exception.
The better question is usually this. What is the lowest-risk plan that protects both maternal functioning and fetal health?
Table of Contents
- Answering the Big Question About Vyvanse and Pregnancy
- What the Latest Research Says About Vyvanse Safety in Pregnancy
- The Hidden Risks of Untreated Maternal ADHD
- ADHD Management by Trimester and for Breastfeeding
- Integrative Alternatives and Support Strategies
- How to Partner with Your Clinician for a Safe Pregnancy
Answering the Big Question About Vyvanse and Pregnancy
A patient takes her usual Vyvanse in the morning, sees a positive pregnancy test that afternoon, and suddenly every dose feels loaded with fear. The first questions are usually immediate and deeply human. Did I already cause harm? Do I need to stop today? How do I make a safe decision without guessing?
The best clinical answer is rarely a simple yes or no. Pregnancy decisions about Vyvanse are usually about risk comparison, not risk elimination. The medication has potential downsides. Untreated ADHD can also create real problems for health, safety, and day-to-day functioning. Good care weighs both sides before changing treatment.
Under the FDA's older system, lisdexamfetamine was classified as pregnancy category C. That label meant animal research had raised concerns and human evidence was limited, so the decision depended on whether the likely benefit to the mother justified possible fetal risk. For patients reviewing treatment paths in more detail, this guide to ADHD medication for pregnant women adds useful context.
Why the old category system left so many patients confused
A single category sounded clearer than it really was. It did not tell patients how severe their ADHD was, whether they could work safely off medication, or how to weigh a small theoretical medication risk against a very real decline in functioning.
Earlier reviews of stimulant use in pregnancy found the human research base was still limited, and much of it focused on first-trimester exposure because that is the period with the greatest concern for structural fetal development. That history helps explain why many pregnant patients still hear conflicting advice from different clinicians.
Practical rule: Avoid panic decisions right after a positive pregnancy test.
In practice, abrupt stopping is often the part I worry about most. Some patients do fine with a pause or taper. Others quickly become less reliable with driving, medication adherence, work demands, sleep routines, or prenatal follow-up. A recommendation that sounds cautious on paper can create new risks if it ignores how that person functions.
A better next step is a structured review with the prescribing clinician and obstetric team. That discussion should cover current dose, symptom severity without medication, past blood pressure issues, sleep, anxiety, substance use history, and whether non-medication supports are enough to keep the patient safe and stable.
That is the key question. Not just, “Is Vyvanse allowed in pregnancy?” but, “What plan gives this specific patient the safest pregnancy overall?”
What the Latest Research Says About Vyvanse Safety in Pregnancy
A patient in early pregnancy often asks one question first: “Did I already hurt the baby?” Research on Vyvanse does not support an automatic assumption of major harm from early stimulant exposure, and that distinction matters in the exam room.
One of the more useful modern data points comes from a 2023 JAMA Psychiatry study summarized in this review of Vyvanse and pregnancy safety. It looked at pregnancies exposed to amphetamine-based ADHD medications, including Vyvanse, and did not find a significant increase in major birth defects.
For patients weighing more than one medication option, this guide to ADHD medication during pregnancy including stimulants and bupropion can help frame the decision.
What looks reassuring
The strongest reassuring signal in the current literature is about major congenital malformations. That is usually the outcome patients fear most, especially after taking medication before they knew they were pregnant.
A large follow-up study also found no increased risk of developmental disorders in exposed children, with an adjusted hazard ratio of 0.97 and a 95% confidence interval of 0.81 to 1.17. That does not prove zero risk. It does mean the available data are more reassuring than many patients expect after reading general warnings online.
What still needs monitoring
The harder part of this conversation is that “reassuring” and “risk-free” are not the same. Current studies are more comforting on birth defects than on other pregnancy outcomes.
Some reports have raised concern about preterm birth, lower birth weight, and maternal blood pressure issues among patients using stimulants during pregnancy. Those findings do not mean Vyvanse directly caused every complication in every study. They do tell clinicians to watch the pregnancy more closely, especially if the patient already has hypertension, poor sleep, anxiety, low appetite, or other obstetric risk factors.
That is the practical framework I use. The question is not only whether the medication has a measurable fetal risk. The question is whether continuing, tapering, or stopping creates the lowest overall risk for this specific patient.
| Area of concern | What the evidence suggests |
|---|---|
| Major birth defects | Large modern data have not shown a significant increase |
| Pregnancy course | Some studies suggest closer monitoring of growth, blood pressure, and timing of exposure |
| Child development later on | Follow-up data have not shown an increased risk of developmental disorders |
Current evidence is more reassuring about major malformations than about blood pressure, growth, and other pregnancy-course outcomes.
That is why a personalized plan matters. Some patients can taper off and function well. Others do better with continued treatment and tighter obstetric monitoring.
The Hidden Risks of Untreated Maternal ADHD
A pregnant patient stops Vyvanse as soon as she sees a positive test. Within two weeks, she is missing prenatal reminders, forgetting to refill another medication, skipping meals because the day gets away from her, and crying in the car after a minor driving mistake. That kind of decline is not rare in clinical practice, and it changes the risk calculation.
Untreated ADHD can interfere with pregnancy care in ordinary, high-impact ways. The problems are often behavioral and logistical rather than dramatic. Missed appointments, poor follow-through, inconsistent sleep, unsafe driving, disorganized medication use, and trouble keeping up with work all affect maternal and fetal health.

When stopping medication creates problems
The practical question is not only whether stimulant exposure carries risk. It is whether stopping treatment creates a different set of risks that may matter just as much for this patient.
For some patients, being off medication means more distraction and a harder workday. For others, functioning drops enough to affect safety and prenatal care.
- Driving safety matters. Distractibility behind the wheel can become a real hazard, especially for patients with long commutes or frequent highway driving.
- Work functioning matters. A lab technician who loses focus while handling specimens or a commercial driver who struggles with sustained attention faces risks that go beyond simple inconvenience.
- Follow-through matters. Forgotten instructions, missed blood pressure checks, or delayed prenatal visits can weaken otherwise appropriate obstetric care.
- Emotional stability matters. Patients who become overwhelmed, panicky, or sleep-deprived after stopping medication may have a harder time managing the rest of pregnancy well.
I often tell patients that functional impairment is a medical issue. It deserves the same attention as blood pressure, nausea, or sleep.
Functional impairment is part of pregnancy risk
Pregnancy is often framed as a time to avoid exposures at all costs. That framing misses an important clinical truth. Maternal functioning is part of fetal protection.
If a patient cannot reliably manage meals, hydration, schedules, transportation, or daily safety, that is not a willpower problem. It is part of the treatment decision. This broader framework for safe ADHD treatment during pregnancy can help patients prepare for a more informed discussion with their obstetric and psychiatric clinicians.
A healthy pregnancy depends on the mother being able to function day to day, not only on avoiding medications.
That same logic applies after delivery. The early postpartum period demands attention, organization, and safe infant care, which is one reason patients often ask practical questions beyond stimulants, including basics like safe cough drops for nursing.
Simple advice such as “avoid it if possible” often fails the patient who becomes chaotic, anxious, and unsafe off medication. In those cases, a supervised plan that accounts for both medication risk and untreated ADHD may be the safer choice.
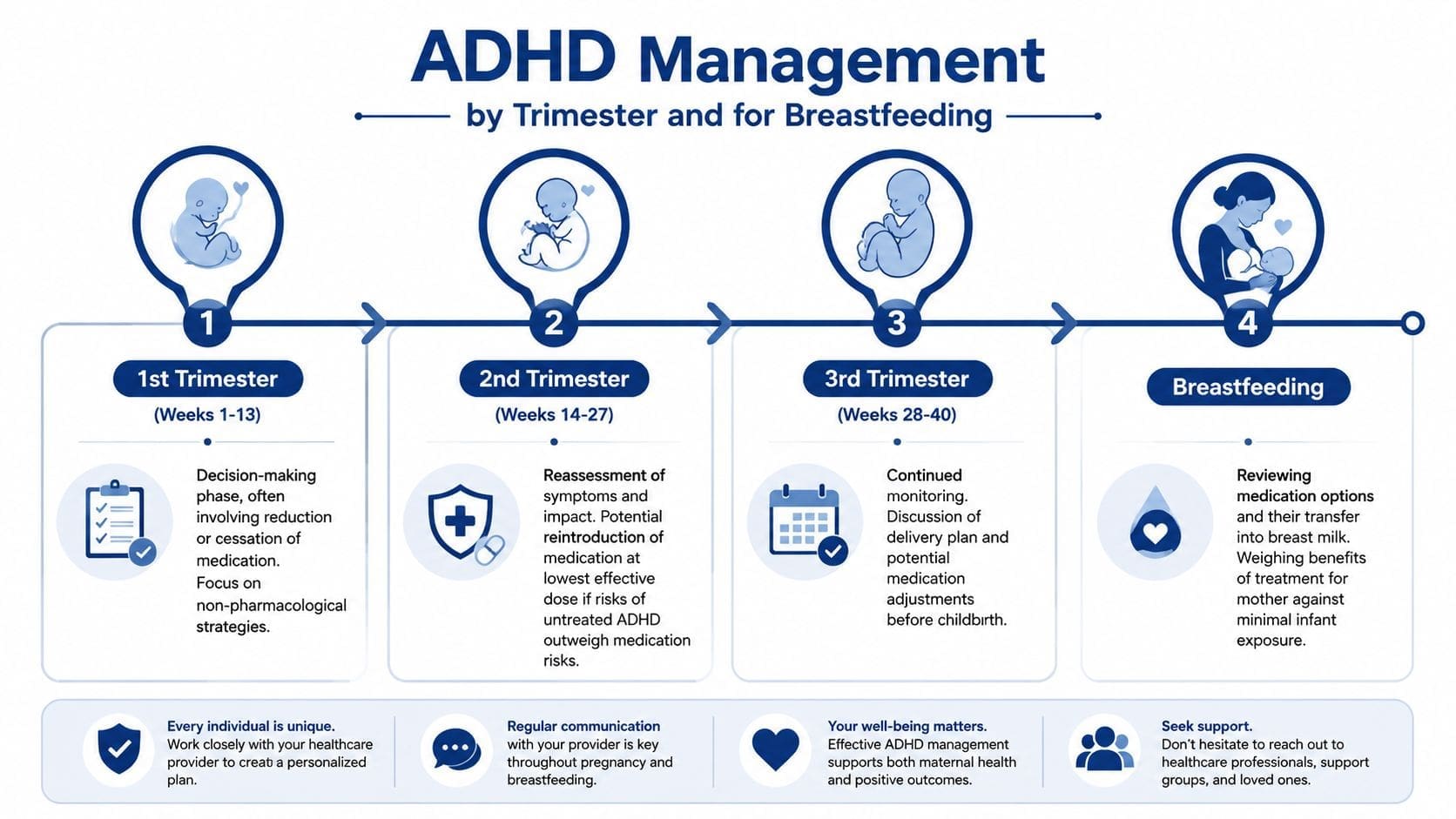
ADHD Management by Trimester and for Breastfeeding
Pregnancy is not one static risk category. The decision often changes as the pregnancy progresses. Timing matters.
Patients looking for a broader decision framework can review safe ADHD treatment during pregnancy alongside discussions with their obstetric and psychiatric clinicians.
First trimester decisions
The first trimester brings the most anxiety because it's the main period of structural development. Many patients discover they were taking Vyvanse before they knew they were pregnant and immediately assume the worst. That reaction is understandable, but it often outruns the data.
What usually helps in the first trimester is a clear review of exposure timing, current dose, symptom severity, and whether tapering or pausing is feasible. Public-facing resources often mention not stopping suddenly, but patients usually need more than that. They need a plan.
A practical first-trimester discussion often includes:
- How much medication was taken and when
- Whether symptoms become unsafe off medication
- What non-medication supports can be added immediately
- How quickly obstetric follow-up can be arranged
Second and third trimester priorities
Later in pregnancy, the focus often shifts. According to BUMPS guidance on lisdexamfetamine, therapeutic amphetamine use is not known to cause birth defects, but later-pregnancy exposure may reduce placental blood flow and increase the chance of low birth weight. Exposure near delivery can also lead to short-term neonatal withdrawal symptoms such as jitteriness, sleep disruption, and feeding or breathing problems.
That changes the clinical conversation.
| Pregnancy stage | Common focus |
|---|---|
| Early pregnancy | Exposure review and decision about continuation, taper, or pause |
| Later pregnancy | Blood pressure, fetal growth, placental blood flow, delivery planning |
Late pregnancy concerns are less about proven teratogenicity and more about growth, blood pressure, and newborn adaptation.
Breastfeeding and postpartum planning
The postpartum period is another pivot point. Some patients plan to breastfeed and also need enough symptom control to function safely with a newborn. That discussion usually includes the pediatrician, obstetric clinician, and psychiatric prescriber.
Medication is only one piece of early postpartum planning. Sleep disruption, feeding schedules, and recovery from delivery all affect ADHD symptoms. Patients often appreciate practical support resources during this stage, even for everyday concerns unrelated to psychiatry. For example, if someone is breastfeeding and sorting through routine symptom relief, this guide on safe cough drops for nursing is a useful example of the kind of cross-checking that helps new parents make safer choices.
Integrative Alternatives and Support Strategies
A pregnancy plan for ADHD often works best when it is built in layers, not around medication alone. The evidence on stimulant exposure is mixed. A systematic review of 12 cohort studies, summarized in this NIH/PMC review on ADHD medication in pregnancy, reported both reassuring findings in some studies and associations with problems such as preeclampsia and NICU admission in others. That uncertainty is exactly why support outside the prescription pad matters.
In practice, the question is rarely, "What can replace Vyvanse perfectly?" The better question is, "What combination of supports lowers risk and keeps daily functioning safe enough?"
Several non-medication strategies can make a meaningful difference:
- ADHD-focused therapy: Skills-based therapy can improve planning, follow-through, and frustration tolerance. It also helps patients prepare for predictable stress points, such as prenatal appointments, work deadlines, and postpartum transitions.
- External structure: Shared calendars, reminder apps, pill organizers, visual checklists, and simplified routines reduce the number of steps a patient has to hold in working memory.
- Nutrition support: Irregular eating can worsen distractibility, irritability, and energy crashes. This guide to nutrition for pregnant women with ADHD offers practical ways to build more consistent meals and protein intake.
- Sleep protection: Sleep loss can sharply worsen ADHD symptoms. Earlier bedtimes, fewer late-evening demands, and partner help with overnight planning can reduce that spiral.
- Pregnancy-safe movement: Gentle exercise often improves restlessness, mood regulation, and sleep.
- Routine cross-checking of everyday products: Patients who are trying to reduce avoidable exposures often benefit from reviewing common over-the-counter items the same way they review prescriptions. Mouthology's recommendations for expecting mothers is one example of that broader safety mindset.
The right mix depends on symptom severity. Someone with mild ADHD may function well with therapy, structure, nutrition, and sleep support during pregnancy. Someone with severe inattention, impulsivity, or functional impairment may still need medication, with close monitoring and a more deliberate risk-benefit discussion.
A good plan also has to fit real life. If a patient works long shifts, drives daily, cares for other children, or has a history of missing important appointments when untreated, those details matter. I would rather see a realistic plan with backup systems than an ideal plan that falls apart within two weeks.
Some patients continue Vyvanse with monitoring. Others taper and rely more heavily on behavioral treatment and environmental supports. Some pause stimulants during one part of pregnancy and revisit the decision later. Integrative Psychiatry of America offers telehealth-based medication evaluation and treatment planning for ADHD in pregnancy as one care option for patients in Pennsylvania.
Support strategies do not erase severe ADHD. They can reduce the load, improve day-to-day stability, and sometimes lower how much medication support a patient needs.
How to Partner with Your Clinician for a Safe Pregnancy
The most productive pregnancy medication visits are specific. Patients don't need to arrive with the right answer. They do need to bring the right details.
What to bring to the appointment
A focused medication review usually goes better when the patient can answer these questions:
- Current use: What dose of Vyvanse is being taken, and how consistently?
- Symptom rebound: What happens on days without it?
- Safety concerns: Is there trouble with driving, job performance, childcare, or missing appointments?
- Medical context: Is there a history of high blood pressure, preeclampsia, or growth concerns in prior pregnancies?
- Support system: Can a partner, family member, therapist, or coach help carry more structure if medication changes?
It also helps to bring a written list of all medications, supplements, and common over-the-counter products. Pregnancy planning is rarely only about one prescription. Even routine self-care items come up. Some patients like practical consumer guidance such as Mouthology's recommendations for expecting mothers when they're reviewing broader pregnancy-safe habits with their care team.
Why telepsychiatry helps
Many patients need specialized ADHD follow-up without adding more travel, waiting rooms, and missed work time to an already stressed schedule. Telepsychiatry makes it easier to have careful medication conversations while staying connected to ongoing care. Patients in Pennsylvania who need follow-up for dosing decisions, taper planning, or symptom monitoring can use online ADHD medication management to keep those check-ins consistent.
A short overview of virtual psychiatric care can help clarify what that process looks like:
The best visit is the one that leads to a clear next step. Sometimes that means continuing medication with monitoring. Sometimes it means tapering. Sometimes it means changing nothing until obstetric input is added. The key is that the plan should be deliberate, documented, and specific to the pregnancy in front of the clinician.
If questions about Can you take Vyvanse while you are pregnant? need a careful, individualized answer, Integrative Psychiatry of America offers confidential telepsychiatry in Pennsylvania for ADHD medication evaluation, pregnancy-related treatment planning, and integrative support strategies that can be coordinated with obstetric care.

