Some people start looking for post traumatic stress disorder therapists after months of telling themselves they should be able to handle it alone. Sleep gets lighter. Crowded stores feel unsafe. A slammed car door, a certain smell, or a late-night phone call can send the body into alarm before the mind catches up. Other people don’t feel keyed up at all. They feel flat, detached, and far away from the people they love.
That pattern is more common than many people realize. In the United States, lifetime prevalence of PTSD reaches 6.8% among adults, and it affects over 13 million people annually, while globally an estimated 3.9% of the population has experienced PTSD at some point, according to the World Health Organization PTSD fact sheet. Those numbers matter for one reason above all. Trauma-related symptoms are not rare, and effective care matters.
PTSD also isn’t a character flaw or a sign that someone is broken. It’s a condition that affects the nervous system, attention, sleep, relationships, and sense of safety. The right treatment can help people feel steadier, more present, and less controlled by what happened to them.
For some people, healing starts with small changes at home. A bedroom that feels calm, predictable, and low-stimulation can support recovery, which is why practical ideas like how to create your perfect sanctuary can be useful alongside clinical care. Environment won’t replace treatment, but it can help the body feel safer between sessions.
Many Pennsylvanians also aren’t sure where to start. They may wonder whether they need a therapist, a prescribing clinician, or both. They may also be asking whether it’s finally time to get professional help. This guide is meant to answer those questions clearly, including when it makes sense to seek specialty care through telepsychiatry and how to decide when to see a psychiatrist.
Table of Contents
- Your Guide to Finding Hope and Healing After Trauma
- Understanding Your PTSD Treatment Team
- Proven Therapeutic Approaches for PTSD Recovery
- Integrating Medication Management into Your PTSD Care
- How to Choose the Right PTSD Therapist in Pennsylvania
- Specialized PTSD Care for Unique Needs
- Questions to Ask a Prospective PTSD Therapist
- Take the First Step Toward Reclaiming Your Life
Your Guide to Finding Hope and Healing After Trauma
The hardest part of PTSD is often how ordinary life stops feeling ordinary.
A parent may sit at a child’s school concert and spend the entire time scanning exits. A nurse may come home from a shift and feel unable to turn off the body’s alarm system. A survivor of assault may want connection and still pull away from touch, conversation, or even eye contact. PTSD can make daily routines feel unpredictable, even when life on the outside looks stable.
That’s one reason people often wait too long to seek help. They assume trauma treatment has to mean retelling every detail immediately, or they worry that opening things up will make symptoms worse. Good treatment doesn’t work that way. Competent post traumatic stress disorder therapists pace the work, build safety first, and use structured methods that reduce overwhelm rather than intensify it.
PTSD treatment works best when the patient feels both challenged and supported. Too much pressure too early usually backfires.
People in Pennsylvania also face practical barriers. Some live in areas with limited specialty care. Some don’t want to sit in a waiting room in their own town. Some work shifts that make weekly commuting unrealistic. Telepsychiatry can remove those barriers while still allowing careful assessment, psychotherapy, medication management when needed, and follow-up that fits real life.
Hope matters here, but false reassurance doesn’t help. PTSD recovery is usually not quick or linear. Symptoms can improve, then flare during stress. Trust may take time. Sleep may improve before relationships do, or the opposite. Progress still counts.
What healing often looks like
Healing usually doesn’t mean forgetting trauma. It means the trauma stops running the day.
That can include:
- Fewer body alarms: less panic, less startle, less scanning for danger.
- Better emotional range: not just less fear, but more access to calm, joy, and connection.
- Improved functioning: sleeping, driving, working, parenting, and leaving the house with less effort.
- More choice: responding to triggers intentionally instead of reacting automatically.
The search for post traumatic stress disorder therapists is often really a search for safety, clarity, and a treatment plan that makes sense. That search gets easier when patients know which professionals do what, and how evidence-based PTSD care is delivered.
Understanding Your PTSD Treatment Team
Different credentials can look confusing fast. The letters matter less than many people think, but the role matters a great deal.

Who does what in PTSD care
Some professionals focus mainly on psychotherapy. Others focus mainly on prescribing. Some can do both.
A simple breakdown helps:
| Professional | Typical focus in PTSD care | Can prescribe medication |
|---|---|---|
| LPC or LMFT | Talk therapy, coping skills, trauma work depending on training | No |
| LCSW | Therapy, case support, trauma-informed counseling | No |
| Psychologist PhD or PsyD | Assessment and psychotherapy | No |
| Psychiatric NP or PMHNP-BC | Assessment, psychotherapy, medication management | Yes |
| Psychiatrist MD or DO | Medical evaluation and medication management, sometimes therapy | Yes |
The phrase trauma-informed care also matters. It means the clinician understands how trauma affects the body, behavior, trust, and treatment engagement. Patients who want a plain-language overview of that framework may find this explanation of trauma-informed care helpful before starting treatment.
The problem for many patients isn’t finding any therapist. It’s finding someone who can treat PTSD with a structured method and also address sleep, panic, depression, concentration problems, or substance use when those issues show up at the same time.
Why a PMHNP can simplify treatment
A Psychiatric-Mental Health Nurse Practitioner, or PMHNP-BC, is trained to assess mental health conditions, provide psychotherapy within scope and training, prescribe psychiatric medication, and monitor how symptoms change over time. For PTSD, that combination can be useful because treatment rarely stays in one lane.
One month the urgent issue may be nightmares. Another month it may be avoidance, emotional numbing, or inability to tolerate therapy homework. A split treatment model can still work well, but it often requires the patient to coordinate between separate providers who may have different impressions or timelines.
A PMHNP-led approach can reduce that fragmentation.
Practical rule: ask whether the clinician treating PTSD can also evaluate sleep, anxiety, depression, substance use, and medication side effects in the same care plan.
That’s also why many patients compare different provider types before booking. A clear explanation of the distinction between prescribing clinicians and therapists can be found in this guide on psychiatrist vs psychiatric NP.
Patients should still ask direct questions. Does the clinician use evidence-based trauma treatment or only supportive talk therapy? Can they recognize when medication might help and when it might distract from the core therapeutic work? Do they understand high-risk occupations, family systems, and cultural stressors that shape trauma responses?
Those questions matter more than credentials alone. The best-fit clinician is the one whose training, scope, and treatment style match the patient’s actual needs.
Proven Therapeutic Approaches for PTSD Recovery
Some therapy helps people feel heard. That matters. But PTSD usually responds best to therapy that is structured, active, and designed specifically for trauma.
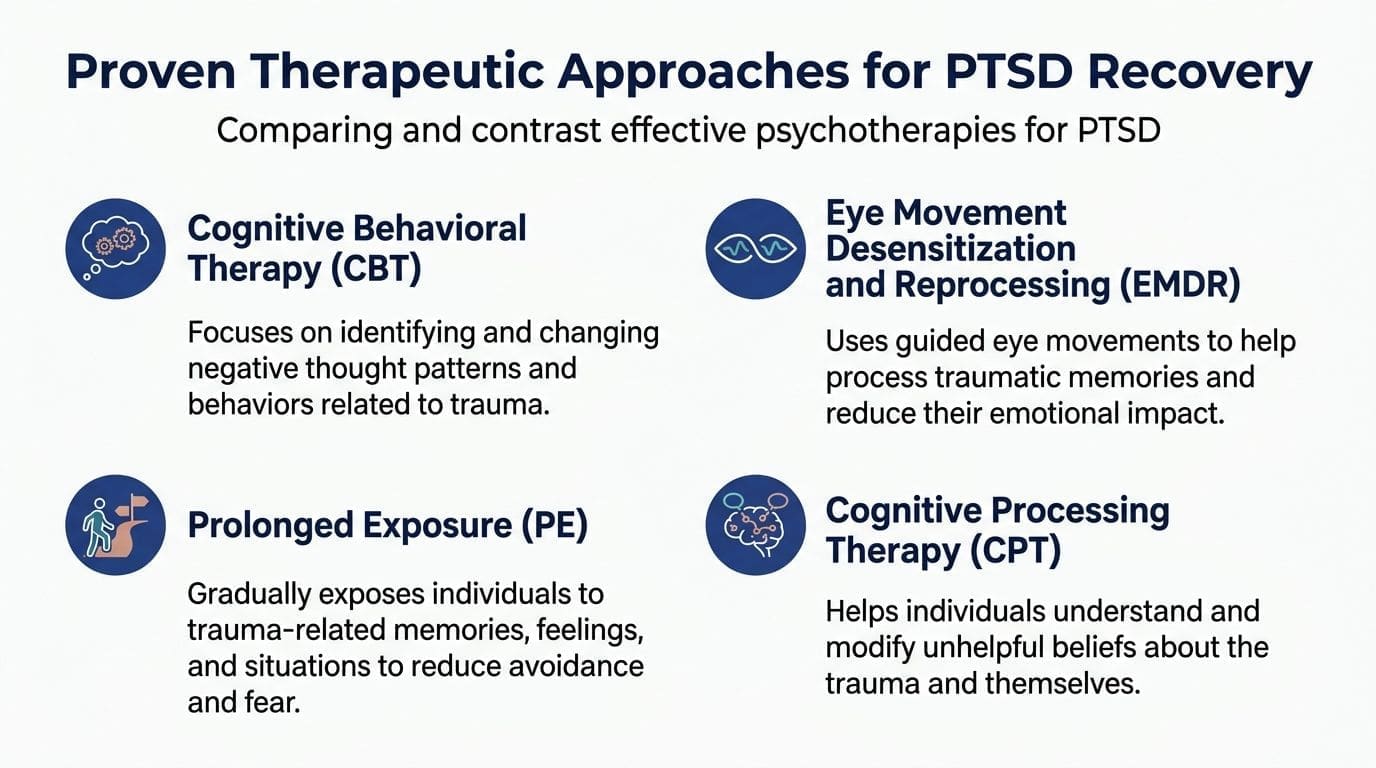
The strongest starting point is straightforward. The VA/DoD Clinical Practice Guideline identifies Prolonged Exposure (PE), Cognitive Processing Therapy (CPT), and Eye Movement Desensitization and Reprocessing (EMDR) as gold-standard treatments, and these manualized therapies are typically completed over 12 to 16 weekly sessions. The same guideline recommends them over first-line medications based on comparative effectiveness research, as outlined by the VA National Center for PTSD overview of trauma-focused psychotherapy.
That recommendation is important because many patients assume medication should come first. For PTSD, that usually isn’t the core strategy. Post traumatic stress disorder therapists who use trauma-focused treatment are trying to change the way the brain and body process the traumatic memory itself, not just soften symptoms around the edges.
Prolonged Exposure PE
Prolonged Exposure is often the best-known therapy that people fear before they understand it.
It helps patients gradually approach memories, feelings, and situations they’ve been avoiding. Avoidance is understandable after trauma, but it teaches the brain that reminders are still dangerous. PE works by helping the brain learn that remembering is not the same as reliving.
A useful analogy is physical therapy after an injury. The goal isn’t to force pain for its own sake. The goal is to restore movement safely, with guidance, repetition, and pacing.
PE often includes:
- Psychoeducation: understanding how PTSD symptoms work.
- In vivo exposure: carefully approaching safe situations that have been avoided.
- Imaginal exposure: revisiting the trauma memory in a structured therapeutic setting.
- Processing: noticing what changes in fear, meaning, and body response over time.
PE isn’t a fit for every patient at every moment. Someone with severe instability, active substance use that prevents participation, or limited coping capacity may need groundwork first. But when done well, it can be highly effective.
Cognitive Processing Therapy CPT
Cognitive Processing Therapy focuses less on fear conditioning and more on the beliefs that harden after trauma.
Many people with PTSD get stuck in thoughts like:
- It was my fault.
- Nowhere is safe.
- I can’t trust anyone.
- My body failed me.
- If I let my guard down, something terrible will happen again.
CPT helps examine those beliefs and test whether they are fully accurate, partly accurate, or trauma-shaped conclusions that no longer serve the patient. This is not forced positivity. It’s disciplined thinking.
Some trauma survivors don’t need to “think positive.” They need help separating what happened from what they came to believe about themselves because it happened.
CPT can be especially useful when shame, guilt, or rigid self-blame are prominent. It gives patients a framework for identifying “stuck points” and replacing them with more balanced interpretations.
EMDR and how memory processing changes
EMDR, or Eye Movement Desensitization and Reprocessing, is often the therapy patients have heard about but don’t fully understand.
In plain terms, EMDR helps the brain process traumatic memories so they become less emotionally charged and less likely to trigger a full alarm response. The therapy uses bilateral stimulation, often guided eye movements, while the patient brings aspects of the traumatic experience into awareness in a controlled way.
Patients often describe the goal as helping the memory feel like something that happened, rather than something that is still happening now.
EMDR can be appealing to patients who struggle to talk through trauma in a highly detailed narrative format. It still requires preparation, trust, and clinical skill. It is not a shortcut, and it should not be marketed as a magical reset.
What works and what tends not to
Not every therapy labeled “trauma therapy” is equally specific.
A practical comparison helps:
| Approach | What it often helps with | Limitation if used alone |
|---|---|---|
| Supportive talk therapy | Feeling heard, relationship support, stress relief | May not fully process trauma patterns |
| General CBT | Anxiety management, coping, behavior change | Can miss trauma-specific beliefs and avoidance loops |
| PE, CPT, EMDR | Core PTSD symptoms and trauma processing | Requires readiness, structure, and trained delivery |
| Medication alone | Sleep, anxiety, mood support | Usually doesn’t resolve the trauma response by itself |
Some patients also ask about broader integrative strategies when PTSD overlaps with depression, anxiety, or treatment-resistant symptoms. That’s where a clinician may review a wider menu of care options, including resources such as ketamine treatment for anxiety and depression in Pennsylvania when clinically appropriate. That isn’t a standard first-line PTSD psychotherapy, but complex cases sometimes require broader psychiatric planning.
The key takeaway is simple. Good PTSD care is not vague. It uses methods with a clear rationale, a defined structure, and a provider who can explain why a given therapy matches the patient’s symptoms.
Integrating Medication Management into Your PTSD Care
Medication has a role in PTSD care, but it works best when patients understand what it can and cannot do.
The treatment hierarchy is clear. The American Psychological Association guidelines strongly recommend trauma-focused psychotherapy as the primary intervention, while pharmacologic treatment such as SSRIs may be considered when patients are unwilling or unable to pursue psychotherapy, or when symptoms continue after therapy. That therapy-first model is summarized in the AAFP review of PTSD guidance.
When medication helps
Medication can reduce barriers that interfere with therapy.
For example, a patient who sleeps only a few hours each night because of nightmares may have trouble concentrating in sessions. Another patient may be so anxious or depressed that starting trauma-focused work feels impossible. In those situations, prescribing can support the larger treatment plan.
Common medication goals in PTSD care include:
- Reducing baseline anxiety and depression
- Improving sleep
- Targeting trauma-related nightmares
- Lowering symptom intensity enough to engage in therapy
Prazosin is sometimes used for trauma-related nightmares. SSRIs and SNRIs may help with mood and anxiety symptoms. Those decisions should be individualized, not automatic.
What integrated prescribing looks like
The trade-off with medication is that symptom relief can be helpful without addressing the underlying trauma pattern. That’s why medication-only care often leaves patients feeling somewhat better but still trapped by avoidance, fear, shame, or emotional disconnection.
A stronger model coordinates prescribing with psychotherapy. A PMHNP can review whether medication is helping the patient attend sessions, tolerate exposure work, sleep enough to function, and notice progress. If a medication is flattening emotion too much, worsening side effects, or creating false expectations, the plan can be adjusted quickly.
This is also where broader evaluation matters. Some patients metabolize medications differently, have past treatment failures, or want more data before trying another option. In selected cases, clinicians may discuss tools such as genetic testing for mental health as one piece of the decision process. It doesn’t replace clinical judgment, but it may inform medication planning.
Medication should support trauma treatment, not replace it by default.
Patients searching for post traumatic stress disorder therapists often don’t realize they may also need a prescriber who understands trauma. The best arrangement is usually the one that keeps the plan coherent. Therapy remains the center. Medication, when used, should make the work more possible.
How to Choose the Right PTSD Therapist in Pennsylvania
The right therapist is not just someone who is kind, available, or covered by insurance. For PTSD, the right therapist is someone who can match training to the patient’s symptom pattern, practical constraints, and readiness for treatment.
PTSD often co-occurs with depression and substance use, and many patients struggle to find therapists trained to handle those complexities. That’s one reason patients benefit from asking targeted questions about personalized care rather than accepting a one-size-fits-all approach, as discussed by the International Society for Traumatic Stress Studies on improving PTSD treatment selection.
What to verify before booking
Start with concrete checks. A polished website isn’t enough.
Use this screening list:
- Confirm the license and role: Know whether the clinician is a therapist, psychologist, PMHNP-BC, or physician prescriber. Scope affects what they can provide.
- Ask about specific PTSD methods: “Do you provide PE, CPT, EMDR, or another structured trauma treatment?” is more useful than “Do you treat trauma?”
- Check comfort with co-occurring issues: If depression, alcohol use, panic, ADHD symptoms, or chronic insomnia are part of the picture, the provider should be able to address that complexity.
- Clarify telehealth logistics: Ask how sessions are conducted, what privacy protections are in place, and how follow-up messages or refill requests are handled.
- Review cost and coverage early: Insurance participation, self-pay rates, and membership models vary. It’s better to know upfront than drop out later over billing confusion.
- Pay attention to fit: Trauma treatment requires trust. If the clinician feels rushed, dismissive, overly rigid, or vague about their method, that matters.
One option for Pennsylvania residents seeking virtual, whole-person psychiatric care is Integrative Psychiatry in PA virtual mental health services. Patients should still compare providers based on training, scope, scheduling, and whether the treatment model matches their needs.
How telepsychiatry changes access across Pennsylvania
Pennsylvania patients often have a very different search experience depending on location.
Someone in Philadelphia may find more clinicians, but also longer waitlists and harder scheduling. Someone in a smaller town may find almost no specialist who treats PTSD with an evidence-based model. Telepsychiatry changes that equation by widening the field of available clinicians across the state.
Telehealth can be especially useful when a patient:
- Needs privacy: local visibility can be a real barrier in small communities.
- Works nontraditional hours: first responders, healthcare workers, and shift employees often need more flexible scheduling.
- Has mobility or transportation barriers: long drives can turn weekly treatment into a burden.
- Feels safer starting at home: some trauma survivors engage better from a familiar environment.
Still, telehealth isn’t automatically easier. The patient needs a private setting, stable internet, and enough emotional safety at home to do the work. A good clinician will ask about those issues rather than assuming virtual care fits everyone equally well.
The strongest choice usually comes down to three things. Proven PTSD training. Clear communication. A plan that fits the patient’s real life in Pennsylvania, not an idealized version of it.
Specialized PTSD Care for Unique Needs
PTSD doesn’t look the same across populations. The symptom categories may be familiar, but the meaning of the trauma, the culture around it, and the practical barriers to treatment can differ sharply.
First responders and high-stress professions
A first responder may not describe trauma the way a civilian would. The language may be operational, practical, or stripped of emotion. Symptoms may show up as irritability, overcontrol, sleep disruption, dark humor, or work-first avoidance, rather than a direct statement like “I’m struggling.”
That difference matters because treatment has to meet the person where they are. A clinician working with emergency physicians, police, firefighters, or paramedics needs to understand the job culture around performance, stoicism, and exposure to repeated distressing material.
Some high-risk groups also face very different probabilities after certain events. Specific traumatic events carry different risks for developing PTSD, including up to 49% of rape victims and 16% of emergency physicians, according to Cross River Therapy’s PTSD statistics summary. Those figures don’t determine any one person’s outcome, but they do support the need for customized, culturally competent treatment.
A provider can know PTSD well and still miss the mark if they don’t understand the patient’s world.
The same principle applies to veterans, LGBTQ+ patients, entertainers, athletes, and people working in public-facing high-pressure roles. Symptoms may overlap. The path into trauma and the barriers to getting help often don’t.
PTSD with co-occurring conditions
Many patients don’t arrive with “just PTSD.”
They may also be drinking too much to sleep. They may have panic attacks, chronic pain, depression, concentration problems, or opioid dependence after an injury. In those cases, trauma care has to be coordinated rather than siloed.
A practical integrated plan may involve:
- Trauma-focused psychotherapy for the PTSD itself
- Medication management for sleep, anxiety, or mood symptoms when needed
- Substance use treatment if alcohol or drug use is interfering with recovery
- Lifestyle support such as exercise, nutrition, and mindfulness when those strategies are realistic and clinically relevant
That integrated approach matters because untreated co-occurring conditions often derail trauma work. A patient can’t fully engage in CPT or PE if they’re sedated every evening, in withdrawal, or sleeping only a few fragmented hours.
Specialized PTSD care isn’t about making treatment look customized for marketing. It’s about recognizing that trauma sits inside a whole life, and the treatment plan has to fit that life.
Questions to Ask a Prospective PTSD Therapist
The first consultation shouldn’t feel like a one-way interview where the patient is being evaluated and has to stay quiet. It should also help the patient evaluate the clinician.
A short list of good questions can reduce anxiety and quickly reveal whether the provider is experienced, structured, and realistic.
A short script for consultations
Patients can ask:
- What experience do you have treating trauma like mine? This matters for assault survivors, first responders, veterans, and patients with medical trauma or repeated loss.
- Which PTSD treatment models do you use most often? A solid answer should include a rationale, not just a list of acronyms.
- How do you decide whether someone is ready for trauma-focused work? Good clinicians assess stability, coping capacity, and safety.
- What happens in the first few sessions? The answer should make the process feel understandable.
- How do you track progress? If the provider can’t explain what improvement looks like, the plan may be too vague.
- How do you handle medication if symptoms are disrupting sleep, focus, or daily function? This is especially important when searching for post traumatic stress disorder therapists who work closely with prescribers or can prescribe themselves.
- How do you treat PTSD when depression or substance use is also present? Many patients need an integrated answer.
This video may help patients think about what trauma treatment conversations can sound like in practice.
A strong consultation doesn’t promise easy healing. It creates clarity. The patient should leave with a sense of the provider’s method, pace, and ability to handle the full picture.
Take the First Step Toward Reclaiming Your Life
PTSD can subtly diminish life. It can narrow relationships, routines, sleep, confidence, and the ability to feel safe in one’s own body. It doesn’t have to stay that way.
Effective treatment exists. The provider matters. The method matters. The fit matters. For many adults in Pennsylvania, telepsychiatry makes it far more realistic to find post traumatic stress disorder therapists or trauma-informed prescribing clinicians who can offer evidence-based care without adding long travel times, local stigma, or unnecessary delays.
Healing usually isn’t about erasing memory. It’s about reducing the grip those memories have on the present. With the right support, patients can move from constant survival mode toward steadier functioning, better relationships, and a wider sense of possibility.
Taking that first step is often the hardest part. It is also the part that changes everything.
If you're looking for confidential online PTSD care in Pennsylvania, IPA Integrative Psychiatry of America offers telepsychiatry with board-certified psychiatric nurse practitioners who provide psychotherapy, medication management when appropriate, and whole-person mental health support. Scheduling a consultation can help clarify the next step.

