Anxiety doesn’t arrive as one clear symptom. It shows up as racing thoughts before bed, a stomach that never settles, irritability that feels out of character, or a constant sense that the nervous system is stuck in “on.” Many adults in Pennsylvania reach a point where they’ve tried standard options, maybe therapy, maybe an SSRI, maybe lifestyle changes, and still feel like the core problem hasn’t shifted.
That’s where interest in low dose naltrexone anxiety treatment has grown. Low-dose naltrexone, usually called LDN, is not a first-line or FDA-approved treatment for anxiety. It is an off-label option. But it has drawn attention in integrative mental health because it appears to work through pathways that are different from conventional anxiety medications, especially pathways involving inflammation, immune signaling, and the body’s own endorphin system.
For the right person, that difference matters. For the wrong person, or with the wrong dosing strategy, it can be frustrating. The practical details matter as much as the theory.
Table of Contents
- A Different Approach to Managing Anxiety in Pennsylvania
- How LDN Works Differently for Anxiety
- Reviewing the Clinical Evidence for LDN and Anxiety
- Potential Benefits and Realistic Expectations
- Navigating LDN Treatment Dosing Risks and Monitoring
- How to Access LDN in Pennsylvania via Telepsychiatry
- Frequently Asked Questions About LDN and Anxiety
A Different Approach to Managing Anxiety in Pennsylvania
A common pattern looks like this. An adult in Pennsylvania starts treatment because anxiety is affecting sleep, focus, patience, and work. Standard treatment helps somewhat, but not enough. The person feels less panicked, maybe, yet still wired, foggy, tense, or physically uncomfortable in a way that doesn’t fit into a single diagnosis.

That experience deserves more than “just keep waiting.” It calls for a broader clinical lens. Integrative psychiatry looks at symptoms, but it also asks what may be amplifying them, such as chronic inflammation, autoimmune illness, disrupted sleep, pain, gut issues, or medication sensitivity.
When standard treatment only partly helps
Some people have clear panic symptoms. Others live with persistent background anxiety that feels more physical than emotional. For many, it helps to start by understanding the symptoms of an anxiety disorder in a more complete way, especially when anxiety overlaps with fatigue, chronic illness, or depression.
In that setting, LDN is worth discussing. It isn’t a replacement for every established treatment. It’s understood as an adjunctive option when the clinical picture suggests that nervous system dysregulation and inflammation may be part of the problem.
Anxiety treatment works best when the plan matches the pattern. A person with trauma, insomnia, pain, and medication sensitivity may need a different strategy than someone with isolated performance anxiety.
Why this conversation is growing
Interest in LDN hasn’t appeared in a vacuum. The World Health Organization estimates that many millions of people live with anxiety disorders and depression, and one review cited by LDN Research Trust noted that 77% of patients using LDN for various chronic conditions reported no ongoing therapy needs, suggesting sustained symptom relief in that broader context (LDN Research Trust overview).
For Pennsylvanians exploring whole-person care, that doesn’t mean LDN is a miracle. It means there is enough signal to justify a thoughtful, safety-focused discussion with a prescribing clinician who understands off-label mental health treatment.
People looking for a broader care model often want support that considers medication, therapy, sleep, nutrition, and medical contributors together. That philosophy is reflected in this overview of integrative psychiatry treatment in Pennsylvania, where the goal is to treat the person, not just the symptom cluster.
How LDN Works Differently for Anxiety
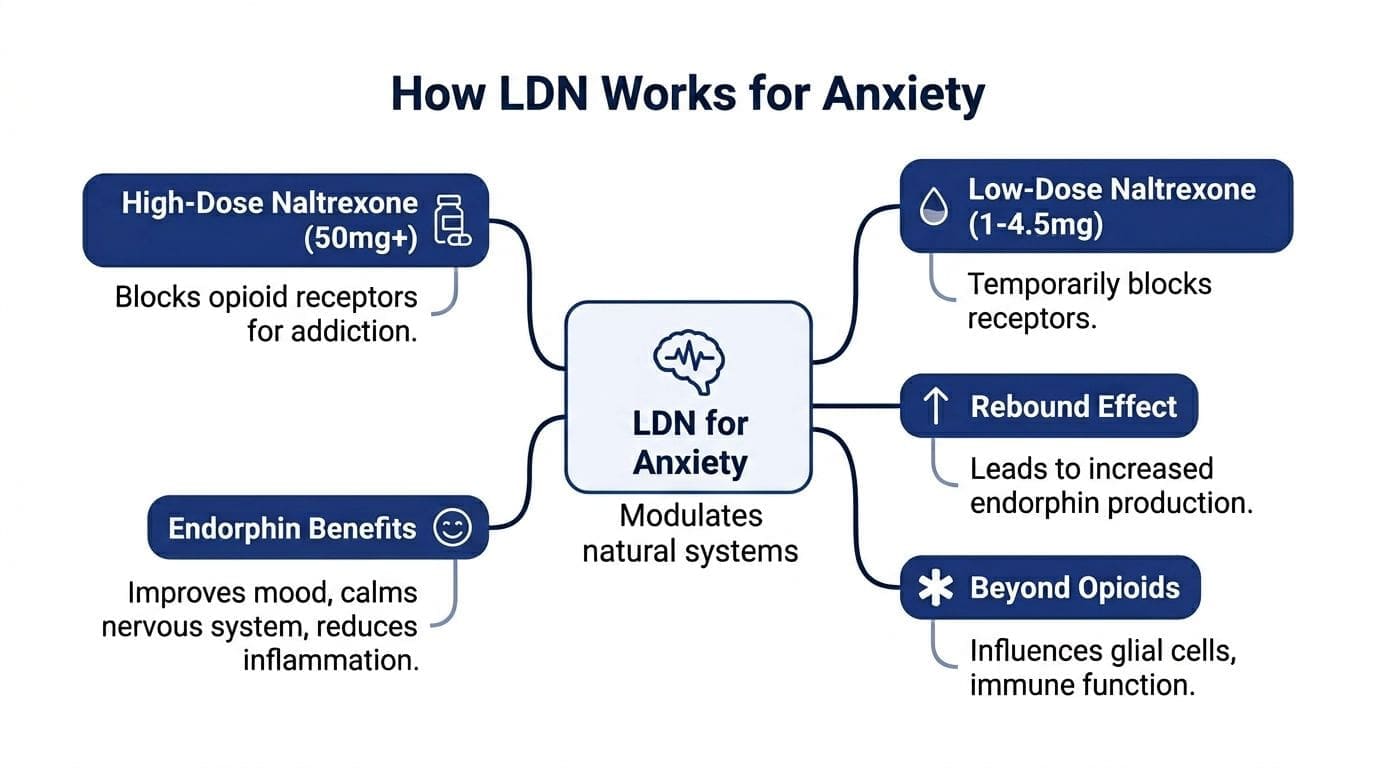
Naltrexone is an older medication. At its standard dosage, it was FDA-approved decades ago for opioid and alcohol dependence. Low-dose naltrexone uses a much lower range, typically a fraction of the standard dose per day, and the effects at that range are not a smaller version of the standard dose.
That distinction matters. High-dose naltrexone acts like a firm blockade. LDN acts like a brief interruption that prompts the body to adapt.
The overnight road closure analogy
A useful way to picture it is this.
High-dose naltrexone is like placing a major roadblock on a highway and keeping it there for a specific purpose. LDN is like a short overnight closure. The temporary interruption signals the system to make adjustments, repair, and compensate. The next day, traffic may move smoothly because the response outlasts the brief closure.
That’s why LDN doesn’t behave like a sedative. It doesn’t directly “knock down” anxiety in the way a benzodiazepine can. Instead, it may help the body regulate itself over time.
The endorphin rebound effect
One proposed mechanism for mood is a brief opioid receptor blockade that triggers the body to increase production of endogenous opioids, including beta-endorphins and enkephalins. These natural signaling molecules are tied to well-being, pain modulation, and emotional resilience.
This matters clinically because many people with chronic anxiety don’t just feel worried. They feel depleted, brittle, reactive, and physically uncomfortable. A treatment that supports endogenous opioid tone may feel less like instant relief and more like improved stress tolerance.
Some clinicians also see this as one reason LDN can be interesting in patients whose anxiety overlaps with pain, post-viral symptoms, fibromyalgia, or autoimmune issues. The symptom clusters often travel together.
The neuroinflammation pathway
LDN appears to work beyond opioid receptors. It acts as an antagonist at Toll-like receptor 4 (TLR4) on microglial cells, the primary immune cells in the central nervous system. That action reduces pro-inflammatory cytokines such as TNF-α, which is why LDN is discussed in relation to neuroinflammation and mood symptoms (review on TLR4 and microglia).
For anxiety, this mechanism is compelling because some patients don’t present like classic serotonin deficiency or isolated anxious thinking. They present like a nervous system that is inflamed, overreactive, sleep-disrupted, and difficult to settle.
Practical rule: LDN makes the most sense when anxiety appears connected to a bigger biological pattern, not when a person is only seeking rapid symptom suppression.
Why that difference matters in real life
People often ask whether LDN is “for anxiety” in the same way an SSRI is for anxiety. Not really. It sits in a different lane.
It may be considered when the treatment goals include:
- Reducing nervous system reactivity instead of chasing short-term sedation
- Supporting mood and pain together when both are present
- Addressing inflammatory contributors when the history points in that direction
- Adding an adjunctive option rather than replacing effective core treatment too quickly
It’s also why LDN works best as part of a broader plan. Sleep hygiene, psychotherapy, exercise, trauma work, and daily tools to regulate your nervous system still matter. LDN doesn’t replace those foundations. It may help some people benefit from them more consistently.
Reviewing the Clinical Evidence for LDN and Anxiety
The research base for LDN and anxiety is promising, but it’s still limited. That’s the most honest summary. LDN is off-patent and off-label, so the literature doesn’t look like the evidence base for newer commercial psychiatric drugs.
Still, there are useful signals. The strongest anxiety-specific point in the available material comes from a Pennsylvania-based study involving people with multiple sclerosis.
What the Pennsylvania study found
A 2022 study in central Pennsylvania looked at people with multiple sclerosis during the early months of the COVID-19 pandemic. Those taking low-dose naltrexone at 2.5 to 4 mg/day had significantly lower anxiety scores on the Hospital Anxiety and Depression Scale-Anxiety subscale than those taking standard oral disease-modifying therapies alone. The difference was statistically significant at p = 0.02, and the proportion scoring at or above the threshold for clinically relevant anxiety also differed significantly at p = 0.016 (study details).
Depression scores were also lower in the LDN plus DMT group than in the oral DMT group in that study. That doesn’t prove LDN treats primary anxiety disorders across the board. It does suggest that in a chronic inflammatory illness, LDN may meaningfully affect mood-related symptoms.
What this means clinically
That study matters because it matches a pattern many psychiatric nurse practitioners watch closely. Anxiety is often louder when chronic illness, inflammation, pain, or immune disruption are part of the picture.
The study also has limits:
- It was a small cohort, not a large multi-site psychiatric trial.
- The population had multiple sclerosis, so the findings can’t be automatically generalized to every person with generalized anxiety disorder or panic disorder.
- It reflects self-reported symptom data, which is useful but not the same as a large blinded trial focused only on anxiety.
Those limits don’t erase the value. They shape how responsibly the data should be used.
Good off-label prescribing starts with honest interpretation. Promising evidence supports consideration. It doesn’t support overclaiming.
Related mood evidence around LDN
Other pieces of the literature help support the broader rationale, even if they aren’t direct proof for primary anxiety disorders. A small study in adults with major depressive disorder used LDN as augmentation for people already on antidepressants and found a reduction in depression severity in relapsers, as summarized in a relevant overview. There is also discussion in the LDN literature of long-term symptom relief across mixed chronic conditions.
A recent randomized controlled trial involving a moderate number of participants found that LDN reduced MADRS depression scores, but placebo showed a comparable reduction. This suggested safety but no superior efficacy as a stand-alone depression treatment, according to an LDN Research Trust summary.
That mixed result is useful. It supports a cautious position. LDN may have value, but it shouldn’t be sold as a proven standalone answer for every anxiety or depression presentation.
For readers wanting a related discussion of mood-focused use, this overview of naltrexone for depression gives additional context about how clinicians think about LDN in psychiatric care.
Potential Benefits and Realistic Expectations
The most common mistake with LDN is expecting it to behave like a rescue medication. It doesn’t. People who do best with LDN tend to understand from the beginning that the target is not instant sedation. The target is steadier regulation.
What benefits people often hope for
LDN’s mood rationale is tied to a paradoxical upregulation of endogenous opioids. Brief receptor blockade signals the body to increase beta-endorphins and enkephalins, creating a rebound effect that may support mood and reduce anxiety without causing dependency, as described in this clinical psychiatry guide on LDN (psychiatry guide).
In practical terms, people interested in low dose naltrexone anxiety treatment are looking for changes like:
- Less background static in the nervous system
- Better emotional resilience under daily stress
- Improved sleep tolerance once the starting phase is handled well
- Reduced overlap with pain or fatigue when those symptoms are part of the same picture
Some also value that LDN is non-addictive and conceptually different from medications that can create dependence concerns.
What it usually does not do
LDN doesn’t provide the fast calming effect associated with a benzodiazepine. It also doesn’t guarantee that anxiety will improve if the main drivers are unaddressed trauma, severe insomnia, stimulant overuse, thyroid imbalance, or a poor medication match elsewhere in the regimen.
That’s why realistic expectations matter. Early benefit feels subtle. Patients may describe fewer spikes, less inner agitation, or a gradual sense that they can recover from stress more easily.
The people most likely to feel disappointed
Three groups struggle with LDN expectations:
| Situation | Why expectations can go off track | Better framing |
|---|---|---|
| Wants instant relief | LDN is not a rapid tranquilizer | Think in weeks, not hours |
| Stopping effective treatment too early | LDN is better as an adjunct | Build around what’s already helping |
| Highly sensitive to medications | Startup effects can overshadow potential benefit | Use slower titration and closer follow-up |
A broader biological view can help here. Anxiety doesn’t always live only in thoughts. It may overlap with pain, immune activation, digestion, and the gut-brain axis, which is why some patients benefit from approaches that also consider inflammation and body-based contributors. This overview of the inflammation gut brain axis explains that connection well.
The most accurate expectation is not “Will this erase anxiety?” It’s “Will this help the nervous system become less reactive and more resilient over time?”
Navigating LDN Treatment Dosing Risks and Monitoring
LDN is one of those medications where the phrase start low and go slow is not a cliché. It’s the treatment strategy. That’s especially true when anxiety patients are sensitive, prone to insomnia, living with trauma, or already taking several medications.
The dose that looks fine on paper can still feel too activating in a real nervous system.
What careful dosing looks like
Some clinical protocols use a low starting point, then increase gradually over periods toward a typical therapeutic range. The best schedule depends on symptom sensitivity, sleep quality, coexisting illness, and what else the patient is taking.
For sensitive patients, clinicians may go much lower. Source material specific to LDN and startup anxiety notes that 0.1 to 0.25 mg can be a reasonable ultra-low starting range when the goal is to reduce the risk of transient worsening or early dropout (clinical discussion of initiation anxiety).
Sample LDN Titration Schedule for Anxiety
| Week | Daily Dose | Common Side Effects to Monitor | Clinician's Action |
|---|---|---|---|
| 1 | 0.1 mg to 0.25 mg | Feeling activated, lighter sleep, vivid dreams, headache | Hold at dose if symptoms are manageable |
| 2 | 0.25 mg to 0.5 mg | Persistent insomnia, increased tension, GI upset | Slow the pace or return to prior tolerated dose |
| 3 to 4 | 0.5 mg to 1 mg | Early morning waking, restlessness, mood fluctuation | Consider morning dosing if sleep is disrupted |
| 5 to 6 | 1 mg to 1.5 mg | Residual activation or no clear benefit yet | Reassess whether the current path still fits |
| Later titration | Gradual increases toward individualized target | Delayed sleep disruption, headaches, overstimulation | Increase only when clearly tolerated |
This is a sample framework, not a universal prescription. Some patients do well with standard titration. Others need to stay at the same dose for longer.
Why some people feel worse at first
A difficult but important truth is that LDN can increase anxiety or disrupt sleep during initiation in sensitive patients. That doesn’t happen to everyone. But when it does, it can make patients quit too early if nobody prepared them for the possibility.
Common early issues include:
- Vivid dreams
- Insomnia
- A brief increase in inner restlessness
- Headaches
Morning dosing may help if nighttime dosing worsens sleep. A slower titration can also make the difference between “this is intolerable” and “this is workable.”
If a patient becomes sharply more activated after starting LDN, the first move usually isn’t to push through aggressively. It’s to reassess timing, dose, pace, and interactions.
Medication interactions and clinical red flags
A critical issue is active opioid use. Because naltrexone blocks opioid receptors, LDN is not appropriate for someone currently relying on opioid medications without a very careful medical plan.
Another practical issue involves thyroid medication. Some guidance notes that LDN may improve thyroid function in certain patients, which can create a mismatch if thyroid medication doses are no longer appropriate. The result can feel like anxiety, palpitations, or overstimulation. That’s one reason symptom changes should never be interpreted in isolation.
Other monitoring points include:
- Current antidepressants or psychiatric medications. Co-prescribing is possible, but it should be reviewed by the prescribing clinician.
- Trauma histories. Patients with reactive nervous systems may need the slowest possible starts.
- Sleep vulnerability. If insomnia is severe, dosing strategy matters more than usual.
Monitoring that helps
Patients do better when the follow-up plan is concrete. Helpful monitoring includes:
- Tracking sleep rather than relying on memory.
- Noting timing of anxiety spikes in relation to dosing.
- Recording dose changes carefully so patterns are visible.
- Reviewing the full medication list whenever side effects appear.
A psychiatric evaluation is especially important when symptoms are complex, persistent, or treatment-resistant. Many adults wait too long before seeking specialty support. This guide on when to see a psychiatrist can help clarify when it makes sense to move beyond self-management and basic primary care prescribing.
How to Access LDN in Pennsylvania via Telepsychiatry
For Pennsylvania adults, the hardest part is not the medication itself. It’s finding a clinician who understands how to evaluate whether LDN fits the full picture and how to prescribe it safely.
Because LDN for anxiety is off-label, the conversation should be thoughtful and specific.

How to prepare for the appointment
Patients get more out of the discussion when they show up with a clear clinical story rather than just asking for a specific prescription.
Helpful preparation includes:
- A symptom timeline that shows when anxiety worsened and what else changed
- A medication list including supplements and thyroid treatment
- Past treatment notes such as which medications helped, which caused side effects, and what happened with sleep
- Relevant medical diagnoses like autoimmune illness, chronic pain, long COVID, fibromyalgia, or digestive issues
A strong question sounds like this: “Could LDN be a reasonable adjunctive option given my anxiety pattern, medication sensitivity, and inflammatory symptoms?”
That framing opens a clinical conversation. It doesn’t force a result.
What a good prescriber should assess
A careful telepsychiatry clinician should review more than anxiety severity. The evaluation should also consider:
- Whether the person is using opioid medications
- Whether sleep disruption is already prominent
- Whether thyroid medication or other medical treatment could complicate titration
- Whether the anxiety pattern suggests a possible inflammatory or chronic-illness component
- Whether LDN should be an adjunct, not a replacement
Experience with integrative mental health matters here. Off-label prescribing shouldn’t mean casual prescribing.
The role of compounding pharmacies
One practical detail surprises many patients. LDN is not commercially available in the low doses used for this purpose, so the prescription usually needs to go to a compounding pharmacy.
A compounding pharmacy prepares the medication in the exact low-dose form ordered by the clinician. That may be a capsule or another formulation depending on the treatment plan. Precision matters because tiny dose adjustments can significantly affect tolerability in sensitive patients.
Why telepsychiatry works well for this process
LDN management benefits from regular check-ins, dose adjustments, and symptom review. Telepsychiatry is well suited to that kind of care because it makes follow-up easier, especially for adults balancing work, parenting, fatigue, or long travel distances within Pennsylvania.
For readers looking into virtual options, this page on integrative psychiatry in PA virtual mental health services outlines how telepsychiatry can support ongoing medication management and whole-person mental health care across the state.
Frequently Asked Questions About LDN and Anxiety
How long until LDN starts helping anxiety
LDN isn't felt as a dramatic same-day change. When it helps, the pattern is gradual. People may notice less reactivity, steadier mood, or better recovery from stress over time rather than instant calming.
Can LDN be taken with an antidepressant
Yes, sometimes, but that decision belongs to the prescribing clinician who has the full medication list. The key issue is not just whether two medications can technically be combined. It’s whether the combination fits the patient’s symptoms, sleep pattern, medical history, and side effect risk.
Is LDN addictive
LDN is not used like an addictive sedative or opioid. In low-dose psychiatric discussions, one reason patients are interested in it is that it may support mood and resilience without the dependency concerns associated with some other anxiety medications.
Why can’t a regular pharmacy just fill it
Because the low doses used for LDN are not standard commercially manufactured doses for this purpose. A compounding pharmacy usually prepares the prescription so the patient receives the exact low dose and titration plan ordered by the clinician.
What if LDN makes anxiety worse at first
This can happen in sensitive patients. It doesn't mean the medication is a poor fit forever, but it means the plan may need adjustment. Common responses include lowering the dose, slowing titration, or switching to morning dosing if sleep is being disrupted.
Adults in Pennsylvania who are curious about low dose naltrexone anxiety treatment need more than generic medication advice. They need a careful evaluation, a realistic plan, and ongoing support from a psychiatric nurse practitioner who understands integrative mental health. IPA Integrative Psychiatry of America provides online psychiatric care across Pennsylvania, including telepsychiatry for anxiety, depression, ADHD, OCD, PTSD, and other complex concerns, with a whole-person approach that considers medication, psychotherapy, nutrition, exercise, mindfulness, and medical contributors to symptoms.

