Your heart is pounding. Your chest feels tight. You keep checking whether you can get a full breath, and the harder you try, the worse it feels. Many adults who search for help with xanax and anxiety attacks are not casually curious. They are trying to get through a frightening moment and want relief fast.
That urgency makes sense. Panic symptoms can feel medical, dangerous, and out of proportion to whatever triggered them. In practice, one of the most important parts of anxiety treatment is honoring both truths at the same time. You need something that helps in the short term, and you also need a plan that protects you in the long term.
The Overwhelming Moment of a Panic Attack
A panic attack rarely feels like “just stress.” It often feels like loss of control.
Someone may be sitting in a work meeting, driving on I-76, or trying to fall asleep when a sudden wave hits. Their pulse surges. Their thoughts jump straight to catastrophe. They may feel detached, shaky, nauseated, or convinced something is terribly wrong.
What patients often describe
In clinical conversations, the pattern is familiar:
- A racing body: Heart pounding, sweating, trembling, shortness of breath.
- A racing mind: “What if I pass out?” “What if this is a heart problem?” “What if I can’t stop this?”
- A shrinking world: Skipping errands, avoiding highways, leaving events early, staying close to “safe” places.
That experience is why Xanax gets so much attention. Xanax, or alprazolam, is known for acting quickly, and when someone feels trapped in the middle of panic, quick relief sounds like the answer they need.
Sometimes it can help. Sometimes it creates a new problem if it becomes the main strategy.
A medication can be useful in a crisis and still be the wrong centerpiece for long-term anxiety care.
Before medication even enters the picture, it helps to have immediate non-drug tools. Breathing practices, grounding, and body-based regulation can lower the intensity of a panic spiral enough for you to think clearly again. If you need a practical starting point, these actionable steps to calm panic attacks offer concrete techniques that many people can use in the moment.
Why the first goal is not perfection
The first goal during a panic attack is not to “win” against anxiety. It is to reduce danger, reduce escalation, and regain enough control to make good decisions.
That includes decisions about medication. Xanax is not a simple yes-or-no topic. It is a fast-acting tool with real strengths, real limits, and real risks. Used thoughtfully, it may help someone get through a rough stretch. Used casually or repeatedly without a broader plan, it can make recovery harder.
How Xanax Quiets the Brain's Alarm System
Anxiety attacks happen when the brain’s threat circuits act like a smoke alarm that has become too sensitive. The system is trying to protect you, but it is firing too hard, too fast, or at the wrong time.
Xanax works by binding to GABA_A receptors, which rapidly suppresses the hyperarousal of an anxiety attack. Effects can begin within 15-30 minutes, with clinical studies showing that 70-90% of patients with panic disorder experience symptom relief within the first week of appropriate, short-term use (understanding Xanax and mental health).
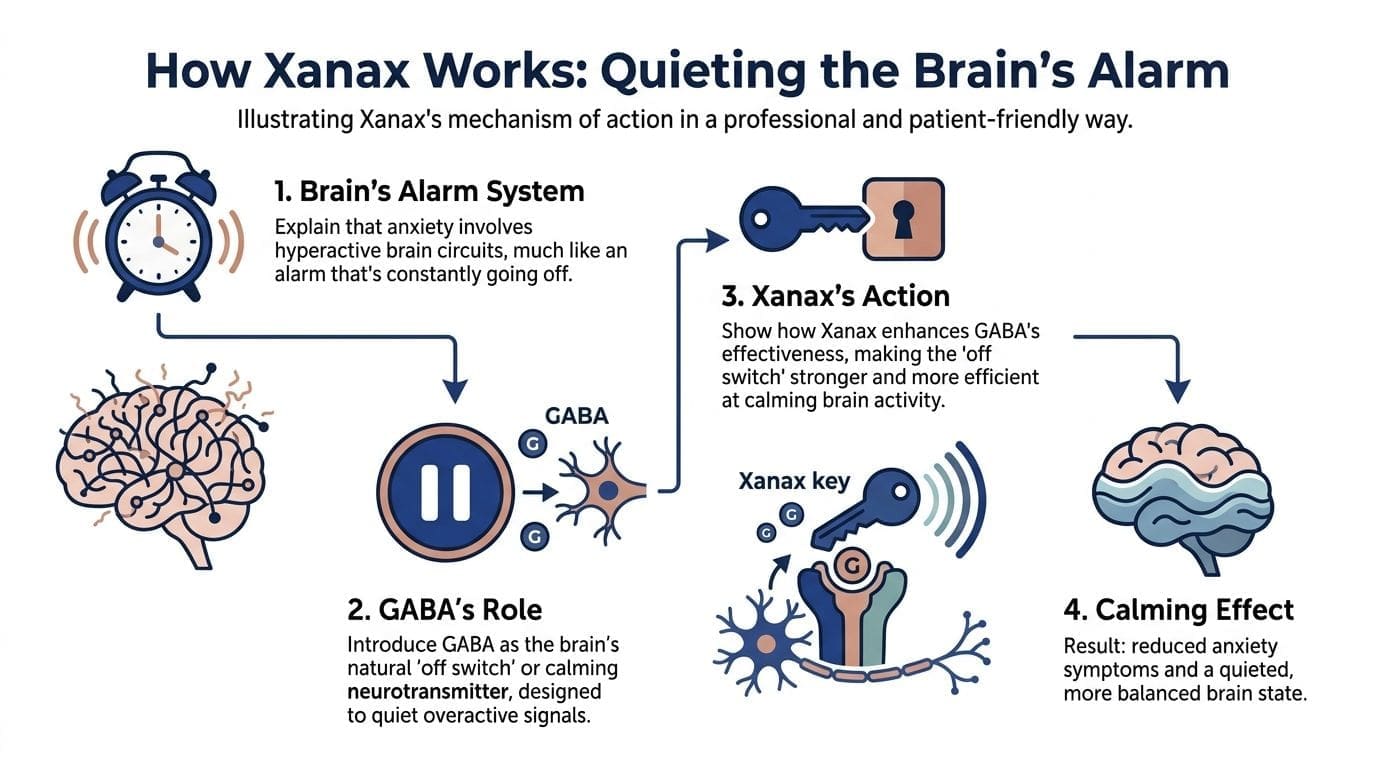
The dimmer switch analogy
The brain uses GABA as one of its main calming signals. If anxiety turns the volume up too high, GABA helps turn it back down.
Xanax does not create calm from nothing. It boosts the effect of GABA, which makes the brain’s built-in braking system work more strongly. For a person in acute panic, that can mean less trembling, less physical activation, and less mental spiraling.
What that feels like in real life
People usually do not describe the effect in technical terms. They say things like:
- “My body stopped surging.”
- “I could finally breathe normally.”
- “The fear backed off enough for me to think.”
That makes sense biologically. When the nervous system is less revved up, symptoms such as muscle tension, racing heart, and shakiness often become less intense. The person is not necessarily euphoric or emotionally “fixed.” They are often just less overwhelmed.
Why timing matters
Part of Xanax’s appeal is speed.
The medication can begin working within 15 to 30 minutes, which is why it is often discussed in the context of panic episodes rather than slow-building, everyday anxiety. It reaches its strongest effect relatively quickly, then fades sooner than many people expect.
That short action window matters. A person may feel relief during the peak of distress, then notice anxiety returning later. For some, that pattern can create a cycle of watching the clock, fearing the return of symptoms, and feeling tempted to rely on repeated doses rather than broader treatment.
Fast relief is useful. Fast relief is not the same as durable recovery.
What Xanax does well and what it does not do
Xanax can be effective for acute symptom suppression. It does not teach your brain how to respond differently to stress, uncertainty, body sensations, or panic triggers.
It also does not address the habits that keep panic alive, such as:
- Avoidance: Leaving places early, canceling plans, staying near exits.
- Body checking: Repeatedly checking pulse, breathing, or dizziness.
- Catastrophic interpretation: Assuming every sensation means danger.
- Sleep disruption: Letting anxiety and poor sleep keep feeding each other.
That is why the most responsible way to think about Xanax is as a short-term intervention that may reduce suffering enough for someone to engage in the important work of treatment. In psychiatric care, the important question is rarely “Can this medication calm panic?” It often can.
The more important question is, “What role should it play, and for how long?”
Using Xanax as a Bridge Not a Destination
When Xanax is used well, it serves a narrow purpose. It helps stabilize a crisis, buys time, and creates enough breathing room for longer-term treatment to start working.
That is the bridge model.
What a bridge looks like
A patient may be dealing with sudden panic attacks, severe anticipatory anxiety, or a short stretch of intense life stress. In that setting, a prescriber may consider Xanax for limited, carefully monitored use while a fuller plan is put in place.
That fuller plan usually includes skill-building and often includes a daily treatment strategy that is safer for ongoing management.
The destination is not “staying calm only if I have Xanax available.” The destination is a life where panic is less frequent, less powerful, and less central to your decisions.
Where people get stuck
Trouble starts when short-term rescue use becomes routine use.
A person takes Xanax for one terrifying episode. Then for a hard week. Then before driving. Then before social events. Then before bed because they are afraid of feeling anxious. At that point, the medication is no longer supporting recovery. It is beginning to organize life around itself.
This is one reason many clinicians also look at non-benzodiazepine supports, daily treatment options, and lifestyle factors that can amplify or soften anxiety symptoms. Even common substances matter. Caffeine, stimulant sensitivity, and calming supplements can shape how “anxious” a body feels across the day. For some patients, this discussion naturally overlaps with topics like L-theanine and caffeine, because nervous system reactivity is rarely about one variable alone.
A better goal
Patients sometimes come in asking for the fastest possible relief. That is understandable. The more useful goal is different: build a treatment plan that makes emergency relief less necessary over time.
Consider the contrast:
| Goal | Likely result |
|---|---|
| Get immediate sedation every time anxiety rises | Short-term relief, higher risk of dependence on rescue medication |
| Build resilience and reduce panic frequency | Slower start, better long-term function and safety |
The bridge model is balanced. It does not demonize Xanax. It also does not romanticize it.
Used briefly and carefully, Xanax may help someone get out of survival mode. But if the bridge becomes the destination, treatment usually stalls. People remain fearful of symptoms, dependent on rapid relief, and disconnected from the tools that change the course of anxiety.
Understanding the Significant Risks of Xanax Use
The same features that make Xanax appealing in a panic emergency also make it risky. It acts quickly, wears off relatively quickly, and can pull people into a pattern of repeated reliance.
Approximately 30.6 million U.S. adults use benzodiazepines like Xanax, but about 5.3 million engage in misuse. From 2003 to 2009, deaths from alprazolam misuse rose by 234%, often due to combination with opioids, highlighting its high potential for addiction and severe consequences (Xanax statistics).

Tolerance and dependence
With repeated exposure, the brain adapts.
A dose that once felt calming may feel less effective later. That can lead people to think they need more frequent use, stronger dosing, or greater psychological reliance on having the medication nearby.
Dependence is not only about misuse in the dramatic sense. It can also develop in people who started with legitimate treatment and gradually became unable to function comfortably without the drug.
Rebound anxiety and withdrawal
One of the hardest clinical realities with Xanax is rebound anxiety. When the medication wears off, anxiety can return with unusual force. Patients may describe this as panic that feels sharper, faster, or more destabilizing than the original problem.
The withdrawal picture can be much worse if someone stops abruptly after sustained use. Symptoms can include severe anxiety, panic, increased heart rate, agitation, tremors, nausea, insomnia, hallucinations, and seizures. In more severe situations, withdrawal can become medically dangerous.
That is why patients should never decide on their own to stop suddenly just because they dislike the medication or want to “get it over with.”
If Xanax has become regular rather than occasional, stopping without supervision can be unsafe.
Dangerous combinations
The most concerning combinations involve other substances that slow the central nervous system.
These include:
- Opioids: This is one of the most dangerous combinations because sedation and breathing suppression can compound.
- Alcohol: Many patients underestimate this risk because alcohol is common and socially accepted.
- Other sedating medications: Sleep aids, muscle relaxants, and some pain medications can increase impairment.
Even if a person does not intend to misuse anything, layering sedating substances can impair judgment, coordination, and breathing. This becomes especially risky when someone is exhausted, emotionally distressed, or trying to self-manage symptoms outside medical oversight.
If substance use, medication misuse, or dual-diagnosis concerns are part of the picture, patients often benefit from integrated psychiatric addiction care rather than treating anxiety in isolation. In that context, services focused on online addiction psychiatry support may be relevant.
Xanax can be dangerous on its own
A common misconception is that Xanax is only risky when mixed with something else. That is false.
Qualitatively, emergency visits related to Xanax often involve the drug by itself. Sedation, impaired coordination, slowed thinking, low blood pressure, and poor balance can all happen without any additional substance involved.
This matters for driving, parenting, decision-making, and work that requires alertness. It also matters for older adults and anyone already prone to falls or confusion.
Rare but serious medical concerns
Most discussions stop at drowsiness and dependence. Patients deserve a fuller picture.
Rare but severe ocular reactions have been reported, including acute angle closure glaucoma after alprazolam exposure. A published case report described bilateral acute angle closure after a single 0.25 mg oral dose, with symptoms including pain and blurred vision within 24 hours (PMC case report on alprazolam and acute angle closure).
That reaction is not common, but it is serious. Sudden eye pain, vision changes, halos, or severe headache after taking a new medication should never be brushed aside.
The practical takeaway
Xanax is not “bad” in a simplistic sense. It is powerful, and powerful medications require disciplined use.
A careful prescriber weighs several questions before continuing it:
- Is this for a short-term crisis or a chronic pattern?
- Is the patient relying on it to avoid learning other anxiety skills?
- Are there substance use risks, medication interactions, or medical vulnerabilities?
- Is the treatment plan moving toward less dependence on rescue medication over time?
If those questions are not being asked, the plan is probably too thin.
Building a Foundation for Lasting Anxiety Relief
Long-term anxiety care works best when it is built on more than symptom suppression. A sustainable plan usually combines medication strategy, psychotherapy, and daily nervous system support.

About 50% of Xanax-related ER visits involve no other drugs, confirming its standalone dangers. In contrast, long-term strategies like psychotherapy and appropriate medication management address the root causes of anxiety, reducing the cycle of panic and dependence seen with short-acting benzodiazepines (can Xanax make anxiety worse).
Daily medications work differently
Many adults assume that if a medication does not work immediately, it must be weaker. That is not how anxiety treatment works.
SSRIs and SNRIs are often used as maintenance treatments because they target anxiety over time rather than producing instant sedation. They are not rescue medications. They are part of a longer arc of treatment aimed at lowering baseline anxiety, reducing panic vulnerability, and making daily life less reactive.
That slower build can feel frustrating early on. But it often supports a more stable outcome because the person is not chasing moment-to-moment relief.
Therapy changes the pattern
Cognitive Behavioral Therapy, or CBT, remains one of the most useful treatments for panic and anxiety because it teaches people how to respond differently to the cycle itself.
That usually includes work around:
- Identifying distorted predictions: “I’m going to pass out” or “I won’t survive this.”
- Reducing avoidance: Returning to driving, stores, crowds, or workouts gradually and purposefully.
- Changing the relationship with body sensations: Learning that a pounding heart or dizziness can be uncomfortable without being dangerous.
- Building response plans: Knowing what to do when panic starts, instead of scrambling.
A pill can reduce a surge. CBT helps reduce the fear of the surge.
Lifestyle care is not optional add-on care
Sleep, movement, nutrition, caffeine intake, alcohol use, and stress load all shape how reactive the nervous system feels. Patients often dismiss these factors because they seem less dramatic than medication. In practice, they matter.
A person who sleeps poorly, consumes high amounts of caffeine, skips meals, and lives in chronic overdrive will usually have a harder time controlling anxiety, even with medication. That is one reason integrative mental health care often includes conversations about how nutrition affects mental health.
Good anxiety treatment is not only about what you take. It is also about what your nervous system has to work with each day.
Short-term relief vs long-term wellness
The trade-offs become clearer when you compare treatment types directly.
| Feature | Xanax (Alprazolam) | SSRIs/SNRIs | Cognitive Behavioral Therapy (CBT) |
|---|---|---|---|
| Main role | Rapid relief during acute anxiety or panic | Ongoing medication management for persistent anxiety patterns | Skill-based treatment for panic, worry, and avoidance |
| Speed of effect | Fast | Gradual | Gradual, with benefits building through practice |
| Best use case | Short-term bridge or occasional rescue use under supervision | Daily treatment plan for long-term anxiety reduction | Long-term change in thinking and behavior patterns |
| Dependence risk | High compared with long-term anxiety strategies | Lower than benzodiazepines in the context of addiction risk | No medication dependence |
| What it changes | Immediate nervous system activation | Baseline anxiety tendency over time | The panic cycle, avoidance, and fear responses |
| Limits | Tolerance, rebound anxiety, withdrawal, interaction risks | Requires patience and follow-up | Requires effort, repetition, and engagement |
For many patients, the best outcomes come from combining a thoughtful medication plan with psychotherapy and behavioral changes, not choosing one camp and rejecting the others.
What sustainable progress often looks like
Improvement is rarely dramatic all at once. It often looks like this:
- Fewer “what if I panic?” decisions.
- Less need to scan the body all day.
- Better sleep.
- More confidence driving, socializing, working, or traveling.
- Less emotional dependence on carrying a rescue medication everywhere.
Later in treatment, educational tools can also help patients understand anxiety physiology and coping. This brief overview may be a useful supplement for some readers:
The most durable anxiety care is rarely flashy. It is structured, repetitive, personalized, and patient. That is what makes it work.
How to Safely Reduce Xanax Use with Your Provider
Do not stop Xanax abruptly. That is the first and most important safety rule.
Withdrawal from Xanax can trigger severe rebound anxiety attacks, panic, and seizures, necessitating a carefully tapered discontinuation plan under medical supervision to avoid symptoms that can be worse than the original anxiety disorder.
What a taper means
A taper is a gradual reduction plan designed by a licensed prescriber. The point is not just to lower the dose. The point is to let the brain and body adjust step by step.
The pace varies. Some people need slower changes because they have taken Xanax regularly, are sensitive to dose shifts, or have other psychiatric or medical factors that complicate the process.
What providers review before tapering
A safe taper starts with a careful clinical review, not guesswork.
That review usually includes:
- Current dose and frequency: Occasional use and daily use are very different situations.
- Duration of use: The longer the pattern, the more carefully the plan usually needs to be built.
- Other medications and substances: Alcohol, sleep medications, opioids, and stimulants all matter.
- Medical and psychiatric history: Seizure risk, severe panic history, trauma, depression, and substance use all shape the plan.
If you are not familiar with the kind of symptom inventory clinicians use to gather a broad picture of health, this overview of a Review of Systems can help you understand why providers ask about symptoms that may seem unrelated at first.
What helps during the taper
People often do better when the taper is paired with active support rather than dose reduction alone.
Helpful supports may include:
- CBT or panic-focused therapy
- Sleep stabilization
- Reducing caffeine and alcohol
- Daily routines that lower nervous system volatility
- A backup plan for breakthrough anxiety that does not default to overuse
If you are unsure whether it is time to involve a specialist in medication management, this guide on when to see a psychiatric provider can help frame the decision.
A taper is not a test of toughness. It is a medical process that should be paced for safety and function.
Find Sustainable Anxiety Control with Telepsychiatry
Adults dealing with panic often need two things at once. They need expert medication judgment, and they need a plan that reaches beyond medication.
That is why telepsychiatry works well for many people with anxiety. It makes follow-up easier, supports consistent monitoring, and removes some of the logistical friction that keeps treatment from becoming steady.

What good anxiety care should feel like
Good care is not just “yes” or “no” to Xanax.
It should feel like a careful assessment of your panic symptoms, your daily anxiety load, your sleep, your medical history, your substance use risk, your goals, and your capacity to engage in long-term treatment. For many adults across Pennsylvania, that kind of consistency is easier to maintain through secure online visits than through fragmented care.
The right endpoint
The healthiest endpoint is not just having a prescription available. It is being less ruled by fear.
That often means:
- Using rescue medication less, not more
- Building confidence in therapy tools
- Choosing daily treatments based on fit and safety
- Strengthening habits that lower baseline anxiety
- Having regular follow-up so adjustments happen early
If you are looking for structured support, anxiety treatment in Pennsylvania with CBT, medication, and telepsychiatry reflects the kind of whole-person model many adults need.
Xanax can be part of anxiety treatment. It should not be the whole treatment. For most patients, the best outcomes come from treating it as a bridge, then building something more durable on the other side.
If you want support from IPA Integrative Psychiatry of America, the next step can be simple. Verify your insurance online, request your initial consultation today, or learn more about anxiety treatment options designed for adults across Pennsylvania. Their telepsychiatry model combines medication management, psychotherapy-informed care, and integrative strategies to help you move beyond crisis relief toward lasting stability.

