Some people looking into topiramate for anxiety are in a very specific place. They have done the responsible things. They tried therapy. They gave an SSRI or SNRI a fair trial. They cut back caffeine, worked on sleep, and still feel keyed up, restless, or stuck in a cycle of panic, hypervigilance, and physical tension.
That frustration is genuine. In practice, this is when patients start asking about medications that are not considered standard first-line anxiety treatment, including Topamax (topiramate). The question is understandable, but the answer needs nuance. Topiramate is not a routine go-to for anxiety, and it is not a simple “yes” or “no” medication. It can help some people. It can also create problems, including making anxiety worse.
When Standard Anxiety Treatments Are Not Enough
A common scenario looks like this. An adult in Pennsylvania starts with a mainstream treatment path for anxiety. They take medication as prescribed, attend therapy, and still wake up with chest tightness, racing thoughts, or an exaggerated stress response that never fully settles.
Sometimes the anxiety is not isolated. It overlaps with trauma symptoms, panic, insomnia, irritability, weight concerns, or a pattern of feeling overstimulated all the time. That matters because persistent anxiety is not always just “anxiety.” It may sit alongside PTSD features, mood symptoms, medical contributors, or medication side effects from prior treatment.
When the usual path falls short
At that point, a careful prescriber may consider options outside the first-line list. That is where topiramate enters the conversation. Not as a first choice. Not as a miracle fix. As one possible tool in a broader treatment strategy when standard approaches have not brought enough relief.
I often encourage patients to think beyond a single pill. If someone has persistent anxiety, I want to know about sleep quality, alcohol use, appetite changes, headaches, trauma history, stimulant intake, and whether there may be medical issues worth ruling out. For some people, a primer on blood tests for anxiety is a useful starting point because thyroid problems, nutrient issues, and other physical factors can overlap with anxiety symptoms.
Clinical reality: Treatment-resistant anxiety usually requires a wider lens, not just a stronger medication.
For patients who need structured care from home, telepsychiatry can make that process much more practical. A thorough anxiety treatment approach in Pennsylvania with CBT, medication, and telepsychiatry can help connect the medication decision to therapy, monitoring, and follow-up instead of reducing the problem to a prescription alone.
What patients need to hear early
Topiramate gets attention because it affects brain signaling in ways that could reduce overactivation. That is the hopeful side. The less discussed side is that some people do poorly on it, especially if they are sensitive to cognitive side effects or prone to worsening mood symptoms.
That is why any discussion of topiramate for anxiety should start with realism. It is an off-label option with mixed evidence, meaningful trade-offs, and a narrow place in treatment. In the right patient, it may be worth considering. In the wrong patient, it can complicate an already difficult picture.
What Is Topiramate and Why Is It Used Off-Label
Topiramate is an anticonvulsant medication. Many people know it by the brand name Topamax. It is commonly recognized for seizure treatment and migraine prevention, which can make its use in psychiatry sound surprising at first.
It is less surprising when you understand how psychiatric prescribing often works. A medication can be approved for one condition and still be prescribed legally for another when a clinician believes there is a reasonable evidence-informed basis to do so. That is called off-label use.
What off-label means
Off-label does not mean experimental in a reckless sense. It means the FDA approval label does not specifically list that condition, even though clinicians may use the medication in real-world practice based on mechanism, smaller studies, clinical experience, and individual patient factors.
Psychiatry uses off-label prescribing regularly. Sleep, trauma symptoms, irritability, intrusive thoughts, and anxiety are all areas where medications sometimes get used outside their original label when standard choices do not fit or have failed.
A related example appears with other neurologic medications discussed in mental health settings, such as Depakote and depression. The principle is similar. The diagnosis on the prescription may not match the drug’s original approval, but the prescribing decision is still based on risk, benefit, and close follow-up.
Why topiramate ends up in anxiety conversations
The reason topiramate comes up is simple. It affects brain excitability. Anxiety often involves a nervous system that feels stuck in “on.” Some patients describe that as internal buzzing, rapid reactivity, hyperarousal, or a body that cannot settle even when the mind wants to.
Topiramate is not a classic antidepressant and not a benzodiazepine. It works through different pathways, and that difference is exactly why some clinicians consider it when usual options have not helped enough.
Here are the settings where it tends to come up most often:
- PTSD with hyperarousal: Especially when intrusive symptoms and physical overstimulation are prominent.
- Social anxiety presentations: Particularly when standard medication trials have been disappointing.
- Complex cases with overlapping neurologic or metabolic concerns: For example, migraine history or situations where weight change matters clinically.
- Adjunctive use: Sometimes it is considered as an an add-on rather than a standalone treatment.
That said, off-label does not equal broadly effective. A medication can be mechanistically interesting and still be a poor fit for many patients. With topiramate, that distinction matters.
How Topiramate May Quiet Overactive Brain Circuits
A patient with severe hyperarousal may tell me, “My body feels like it never turns off.” In cases like that, the question is not whether topiramate is a calming medication in a broad sense. The question is whether it can reduce the specific pattern of overactivation driving the symptoms, without creating new problems that outweigh the benefit.
Topiramate affects several signaling systems involved in excitability. That is the main reason it enters anxiety discussions, especially in patients whose symptoms look less like persistent worry and more like a brain and body stuck in high alert.
The inhibitory pathways it may strengthen
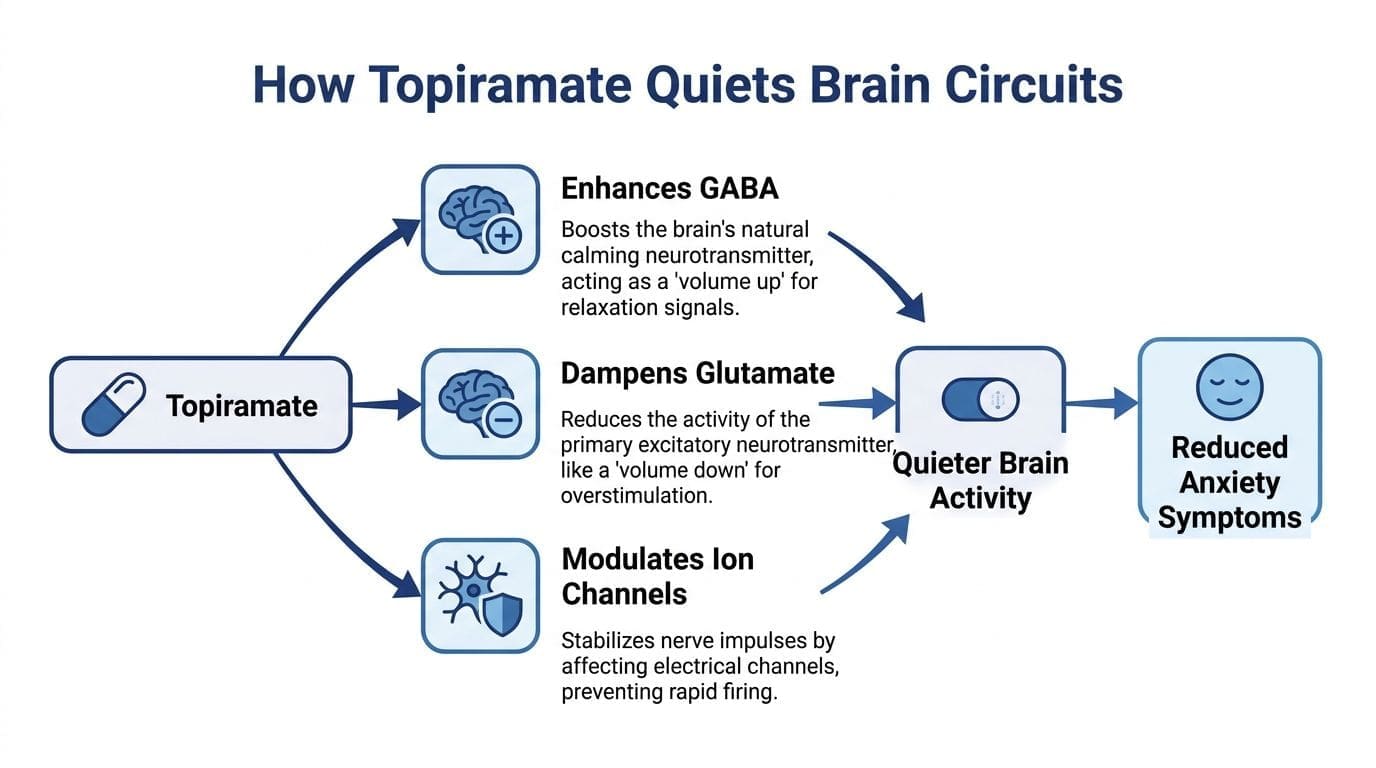
One proposed mechanism involves GABA, the brain’s main inhibitory neurotransmitter. GABA helps regulate firing and prevent circuits from staying overactive. Topiramate appears to enhance inhibitory signaling at GABA-A receptors, which may help some patients feel less keyed up, less reactive, and less physically activated.
That explanation is useful only if it connects to symptoms I can monitor in the clinic. The patients most likely to fit this model are usually describing internal overstimulation, rapid startle, sensory overload, or a body that stays braced long after a stressor passes.
The excitatory pathways it may dampen
Topiramate also blocks AMPA/kainate glutamate receptors, which may reduce excessive excitatory firing in some brain circuits linked to arousal. It has additional effects on sodium and calcium channels, which may further stabilize neuronal signaling.
In practical terms, that can matter for people with trauma-related reactivity, racing mental speed, or a “too loud” nervous system. It does not mean the medication is broadly soothing. It means there is a biologic rationale for trying it in selected patients whose anxiety has a strong hyperarousal component.
This is also where clinical caution matters. A medication that lowers excitability in one person can feel mentally dulling, disorganizing, or emotionally unsettling in another. In my practice, that trade-off is part of the discussion from the start, because cognitive slowing or a strange “off” feeling can increase distress and, in some patients, make anxiety worse rather than better.
For patients who want to look beyond medication alone, our discussion often includes how inflammation and the gut-brain axis can shape mood and stress reactivity. Sleep disruption, chronic stress, nutrition, alcohol use, trauma load, and migraine patterns can all influence whether topiramate is even the right tool.
What this can look like clinically
The mechanism matters only if it maps onto a specific symptom pattern. In practice, topiramate is usually considered for symptoms such as:
- Hyperarousal: feeling jumpy, on edge, or easily triggered
- Racing thoughts: mental overactivation that does not settle well
- Physical tension: internal restlessness, clenched muscles, jaw tension, or a revved-up body
- Trauma-linked reactivity: exaggerated startle, intrusive activation, or a persistent defensive state
Key takeaway: Topiramate is being considered for its effects on excitability and arousal circuits, not because it works like a first-line anxiety medication.
That distinction protects patients from a common mistake. Mechanistic logic can sound persuasive, but it is not the same as reliable symptom relief. With topiramate, the practical question is always whether the patient feels calmer and more functional, or more anxious, foggy, and uncomfortable once treatment begins.
Reviewing The Clinical Evidence For Anxiety and PTSD
A common clinical scenario is the patient with PTSD or severe anxiety who has already tried standard options, still feels keyed up, and asks whether topiramate is the next logical step. My assessment is simple. The evidence is interesting, limited, and easy to oversell.
PTSD data suggests a signal, but not a reliable win
PTSD is one of the main areas where topiramate has been studied for off-label psychiatric use. A commonly cited review summarizes a randomized, placebo-controlled trial in adults with non-combat PTSD. In that study, topiramate showed larger numerical improvements than placebo across total PTSD symptoms and symptom clusters such as reexperiencing, avoidance, and hyperarousal, but the overall difference on total CAPS scores was not statistically significant (National Depression Hotline summary of topiramate and anxiety research).
That distinction matters in practice. Numerical improvement can justify clinical interest. It does not justify presenting topiramate as an established anxiety treatment.
For patients with trauma symptoms, I put the focus on a broader PTSD treatment approach that includes therapy and nervous system stabilization. Medication may reduce symptom intensity for some people, but it rarely carries recovery by itself.
Why the evidence has not changed routine practice
Guidelines remain cautious for good reasons. The studies are small, the results are mixed, and tolerability affects whether a patient can stay on the medication long enough to see any benefit.
This is also where online discussions often lose the plot. They highlight that topiramate may help hyperarousal or intrusive symptoms, then gloss over the fact that some patients stop it early because they feel cognitively slowed, physically uncomfortable, or emotionally worse. For an anxious patient, that is not a side issue. It changes the whole risk-benefit calculation.
A medication with limited evidence and meaningful dropout rates belongs in a select-case conversation, not in a routine first-line plan.
The practitioner's reality check
The most under-discussed point is patient safety. Topiramate may help a subset of patients with trauma-linked overactivation, but I have to weigh that against another distinct possibility. It can increase distress in some individuals, especially if the person is sensitive to medication effects or becomes unsettled by feeling slowed down, foggy, or unlike themselves.
That is why I read this evidence conservatively. Topiramate remains an off-label option that may deserve consideration in carefully selected cases of PTSD or difficult-to-treat anxiety. It does not have the consistency, tolerability, or predictability of standard first-line treatments, and it should never be framed as an easy answer.
Common Side Effects and The Risk of Worsening Anxiety
A common office scenario goes like this. A patient starts topiramate hoping it will quiet anxiety, then returns saying, “I feel foggy, keyed up, and not like myself.” That response is not rare enough to dismiss, and it is one reason I discuss this medication more cautiously than many online summaries do.

Topiramate can help some patients, but it can also increase distress. Clinical references and prescribing experience both support that concern. Anxiety may rise directly, or it may worsen indirectly because the person feels cognitively slowed, physically strange, or emotionally flattened. That distinction matters in practice, because the patient still feels worse either way.
The under-discussed safety issue is straightforward. A medication considered for anxiety can aggravate anxiety.
I pay close attention to that risk in patients who already have a fragile baseline. The pattern shows up more often in people who are highly sensitive to medication effects, prone to panic about bodily sensations, dealing with depression or irritability, or working in roles where even mild word-finding difficulty creates immediate stress.
Psychiatric side effects deserve equal billing
Patients often expect an anxiety medication to feel calming or at least emotionally neutral. Topiramate does not reliably behave that way. Some people report more inner tension, more irritability, sleep disruption, or a detached feeling that they find unsettling rather than relieving.
Those reactions can feed anxiety fast. Anxious patients tend to notice internal changes early, and they may interpret cognitive slowing, tingling, dizziness, or appetite changes as signs that something is wrong. Once that cycle starts, the medication itself can become part of the symptom burden.
If anxiety worsens after starting topiramate, I do not frame that as something to tolerate for weeks. It calls for reassessment of dose, pace of titration, overall fit, and whether the medication should be stopped.
Common side effects patients notice first
The side effects that most often shape day-to-day tolerability are familiar:
- Paresthesia: tingling in the hands, feet, or face
- Cognitive slowing: brain fog, slower processing, or trouble finding words
- Fatigue
- Dizziness
- Insomnia
- Taste changes
- Reduced appetite
Word-finding problems deserve special attention. For students, attorneys, teachers, executives, clinicians, and anyone who relies on quick verbal recall, that side effect is not minor. It can create embarrassment, reduce work performance, and increase anxiety about functioning.
A separate point often gets overlooked. Topiramate is not a substitute for every type of anxiety treatment need. Patients comparing a daily off-label medication with as-needed options should understand the trade-offs, especially if they are also considering approaches for acute episodes such as Xanax and anxiety attacks. In other cases, a non-benzodiazepine option like propranolol for anxiety may be discussed for specific physical symptoms, though that serves a very different role than topiramate.
Why dose changes need patience
Topiramate usually becomes harder to tolerate when the dose rises too fast. Slow titration is part of safe prescribing, not a technical detail. Starting low gives patients and clinicians time to separate a temporary adjustment effect from a pattern that signals poor fit.
A brief overview is helpful here:
Weight loss is another reason some patients ask about topiramate. Some people see that as a benefit, especially when weight gain from other psychiatric medications has been frustrating. I still caution against chasing that effect. A medication that lowers appetite but leaves the patient more anxious, more depressed, or less mentally sharp is not helping the larger treatment plan.
The safest use of topiramate for anxiety includes careful screening, slow titration, early follow-up, and clear stop rules. If mood drops, anxiety climbs, or cognition changes enough to disrupt work or daily life, the plan should change quickly. At Integrative Psychiatry of America, I want patients to understand these considerations before trying an off-label option that can either help or clearly backfire.
Comparing Topiramate Against Standard Anxiolytics
Topiramate makes the most sense when patients understand where it sits relative to standard anxiety medications. It is not competing on equal footing with first-line options. It occupies a narrower, more selective role.
Topiramate vs standard anxiety medications at a glance
| Feature | Topiramate (Off-Label) | SSRIs/SNRIs (e.g., Lexapro, Zoloft) | Benzodiazepines (e.g., Xanax, Klonopin) |
|---|---|---|---|
| Primary role in anxiety care | Considered in select, complex cases | Common first-line treatment | Short-term or situational relief in selected cases |
| Mechanism | Modulates GABA, glutamate, and ion channels | Primarily acts through serotonin or serotonin/norepinephrine pathways | Enhances GABA signaling more directly |
| Best fit | Patients with unusual treatment needs, trauma-linked hyperarousal, or specific comorbid patterns | Broad anxiety disorders with ongoing symptoms | Acute panic, short-term bridging, or limited targeted use |
| Main drawbacks | Cognitive slowing, tingling, mood worsening, possible anxiety worsening | Sexual side effects, GI issues, activation in some patients, withdrawal symptoms if stopped abruptly | Sedation, tolerance, dependence, memory problems |
| Dependency risk | Not typically thought of as habit-forming in the way benzodiazepines are | Not considered addictive, though discontinuation can be difficult | Meaningful dependence risk |
| Weight effects | May reduce appetite or weight in some patients | Varies by medication | Often neutral, but can indirectly affect energy and activity |
| How fast it feels different | Variable and often limited by the need for slow titration | Usually gradual | Often rapid |
The practical trade-offs
SSRIs and SNRIs remain first-line because they have a much broader evidence base for panic disorder, generalized anxiety disorder, social anxiety, and related conditions. They are imperfect, but they are familiar, studied, and effective enough to justify starting there.
Benzodiazepines work differently. They can provide fast relief, but the price is higher risk around dependence, sedation, and long-term difficulty. Some patients looking for help with physical symptoms of anxiety may also ask about alternatives like propranolol for anxiety, which is another example of how treatment should match symptom pattern rather than defaulting to one drug class.
Where topiramate fits
Topiramate stands apart because it is neither a standard daily antidepressant approach nor a classic rapid-relief medication. That can be useful in a narrow subset of patients. It can also leave patients disappointed if it is presented as a mainstream anxiety treatment when it is not.
A good prescribing discussion compares medications by what patients care about:
- Will I think clearly on it?
- Will it make me calmer or stranger?
- Does it help panic, trauma hyperarousal, or social anxiety?
- What happens if my mood drops?
- Is the side effect profile workable for my job and life?
That level of comparison is more useful than calling one medication “stronger” than another.
Who May Be a Candidate for Topiramate Therapy
Topiramate is a selective option, not a broad recommendation. The best candidates tend to have a specific reason to consider it, not just a desire to try something different.
Profiles where it may be worth discussing
A topiramate trial may be reasonable when the clinical picture includes one or more of the following:
- Standard anxiety treatment has fallen short. The person has had an adequate trial of more conventional approaches and still has significant symptoms.
- PTSD features are prominent. Hyperarousal, startle, reexperiencing, or trauma-linked physiologic activation may make the mechanism more relevant.
- Migraine prevention is also a treatment goal. In some patients, one medication addressing more than one issue can simplify care.
- Weight change matters clinically. This should be a secondary consideration, not the main reason, but it can influence decision-making in some cases.
- The person is willing and able to monitor closely. This is not a good medication for someone who wants a set-it-and-forget-it approach.
People who should think twice
Topiramate is a poor fit when certain risks are already present.
A cautious prescriber will pause if the patient has:
- A history of cognitive side effects from medication
- Work that depends on rapid verbal fluency or precision
- A pattern of worsening depression, irritability, or agitation on psych meds
- Kidney stone history or other medical reasons for caution
- Pregnancy or plans to become pregnant
- An eating disorder or a situation where appetite suppression would be harmful
Decision guide: A medication can be pharmacologically interesting and still be the wrong choice for your actual life.
Questions worth asking before starting
A thoughtful consultation should cover questions such as:
- What anxiety symptoms are we trying to target specifically?
- Why are we choosing this over an SSRI, SNRI, or another approach?
- How will we know early if it is helping?
- What side effects mean “monitor,” and which mean “stop”?
- How will this affect work, concentration, and sleep?
If those questions are not getting answered, the treatment plan is probably not specific enough.
Building Your Integrative Anxiety Treatment Plan
Medication decisions work best when they sit inside a larger plan. That is especially true with topiramate for anxiety, because success depends on much more than the prescription itself.
Topiramate does not teach nervous system regulation. It does not process trauma. It does not fix chronic sleep deprivation, heavy alcohol use, poor nutrition, or a daily routine built around overstimulation. It may help some people, but it cannot carry the entire treatment burden.
What a strong plan usually includes
The most effective anxiety care is layered.
A practical integrative plan combines:
- Medication management: With a clear target symptom list and follow-up schedule.
- Psychotherapy: CBT, trauma-focused work, exposure therapy, or skills-based treatment depending on the diagnosis.
- Sleep intervention: Because insomnia can imitate medication failure.
- Exercise and nervous system regulation: Regular movement changes baseline arousal more than many patients expect.
- Nutrition support: Blood sugar instability, heavy stimulant use, and poor intake can all amplify anxiety.
- Mindfulness or breathwork: Not as a cure-all, but as part of reducing chronic activation.
How to talk with your prescriber about topiramate
Patients do best when they come prepared. Bring a short symptom history. List medications you have already tried and what happened on each one. Be specific about whether the main issue is panic, trauma symptoms, social anxiety, insomnia, irritability, or nonstop physical tension.
Then ask direct questions:
- What is the goal of using topiramate in my case?
- Why are we choosing this over an SSRI, SNRI, or another approach?
- How will we know early if it is helping?
- What side effects mean “monitor,” and which mean “stop”?
- How will this affect work, concentration, and sleep?
What works best over time
The patients who tend to do best are not the ones chasing a perfect medication. They are the ones building a treatment system. They track symptoms. They report side effects early. They stay engaged in therapy. They adjust sleep, stress load, movement, and substance use patterns while the medication plan is being refined.
That is an important consideration with topiramate. It may have a place. It is rarely the whole answer.
If you live in Pennsylvania and want a thoughtful, whole-person approach to anxiety care, IPA Integrative Psychiatry of America offers online psychiatric evaluation, medication management, and integrative treatment planning suited to your symptoms, history, and goals. A careful assessment can help determine whether topiramate belongs in your plan or whether a safer, more effective path makes better sense for your situation.

